

Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
134<br />
Laparoscopic Appendectomy in the Third Trimester of Pregnancy: Report of Two Cases ...<br />
<strong>June</strong> <strong>2011</strong><br />
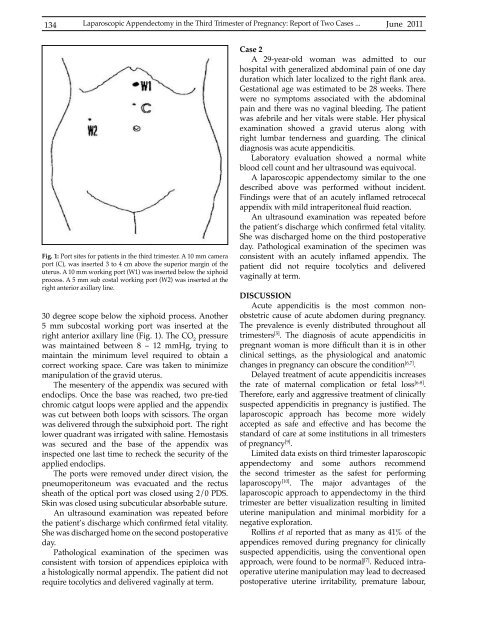
Fig. 1: Port sites for patients in the third trimester. A 10 mm camera<br />
port (C), was inserted 3 to 4 cm above the superior margin of the<br />
uterus. A 10 mm working port (W1) was inserted below the xiphoid<br />
process. A 5 mm sub costal working port (W2) was inserted at the<br />
right anterior axillary line.<br />
30 degree scope below the xiphoid process. Another<br />
5 mm subcostal working port was inserted at the<br />
right anterior axillary line (Fig. 1). The CO 2<br />
pressure<br />
was maintained between 8 – 12 mmHg, trying to<br />
maintain the minimum level required to obtain a<br />
correct working space. Care was taken to minimize<br />
manipulation of the gravid uterus.<br />
The mesentery of the appendix was secured with<br />
endoclips. Once the base was reached, two pre-tied<br />
chromic catgut loops were applied and the appendix<br />
was cut between both loops with scissors. The <strong>org</strong>an<br />
was delivered through the subxiphoid port. The right<br />
lower quadrant was irrigated with saline. Hemostasis<br />
was secured and the base of the appendix was<br />
inspected one last time to recheck the security of the<br />
applied endoclips.<br />
The ports were removed under direct vision, the<br />
pneumoperitoneum was evacuated and the rectus<br />
sheath of the optical port was closed using 2/0 PDS.<br />
Skin was closed using subcuticular absorbable suture.<br />
An ultrasound examination was repeated before<br />
the patient’s discharge which confirmed fetal vitality.<br />
She was discharged home on the second postoperative<br />
day.<br />
Pathological examination of the specimen was<br />
consistent with torsion of appendices epiploica with<br />
a histologically normal appendix. The patient did not<br />
require tocolytics and delivered vaginally at term.<br />
Case 2<br />
A 29-year-old woman was admitted to our<br />
hospital with generalized abdominal pain of one day<br />
duration which later localized to the right flank area.<br />
Gestational age was estimated to be 28 weeks. There<br />
were no symptoms associated with the abdominal<br />
pain and there was no vaginal bleeding. The patient<br />
was afebrile and her vitals were stable. Her physical<br />
examination showed a gravid uterus along with<br />
right lumbar tenderness and guarding. The clinical<br />
diagnosis was acute appendicitis.<br />
Laboratory evaluation showed a normal white<br />
blood cell count and her ultrasound was equivocal.<br />
A laparoscopic appendectomy similar to the one<br />
described above was performed without incident.<br />
Findings were that of an acutely inflamed retrocecal<br />
appendix with mild intraperitoneal fluid reaction.<br />
An ultrasound examination was repeated before<br />
the patient’s discharge which confirmed fetal vitality.<br />
She was discharged home on the third postoperative<br />
day. Pathological examination of the specimen was<br />
consistent with an acutely inflamed appendix. The<br />
patient did not require tocolytics and delivered<br />
vaginally at term.<br />
DISCUSSION<br />
Acute appendicitis is the most common nonobstetric<br />
cause of acute abdomen during pregnancy.<br />
The prevalence is evenly distributed throughout all<br />
trimesters [5] . The diagnosis of acute appendicitis in<br />
pregnant woman is more difficult than it is in other<br />
clinical settings, as the physiological and anatomic<br />
changes in pregnancy can obscure the condition [6,7] .<br />
Delayed treatment of acute appendicitis increases<br />
the rate of maternal complication or fetal loss [6-8] .<br />
Therefore, early and aggressive treatment of clinically<br />
suspected appendicitis in pregnancy is justified. The<br />
laparoscopic approach has become more widely<br />
accepted as safe and effective and has become the<br />
standard of care at some institutions in all trimesters<br />
of pregnancy [9] .<br />
Limited data exists on third trimester laparoscopic<br />
appendectomy and some authors recommend<br />
the second trimester as the safest for performing<br />
laparoscopy [10] . The major advantages of the<br />
laparoscopic approach to appendectomy in the third<br />
trimester are better visualization resulting in limited<br />
uterine manipulation and minimal morbidity for a<br />
negative exploration.<br />
Rollins et al reported that as many as 41% of the<br />
appendices removed during pregnancy for clinically<br />
suspected appendicitis, using the conventional open<br />
approach, were found to be normal [7] . Reduced intraoperative<br />
uterine manipulation may lead to decreased<br />
postoperative uterine irritability, premature labour,













