

Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
128<br />
The Diagnostic Value of Sinus-Track Cultures in Secondary Pediatric Chronic Osteomyelitis<br />
<strong>June</strong> <strong>2011</strong><br />
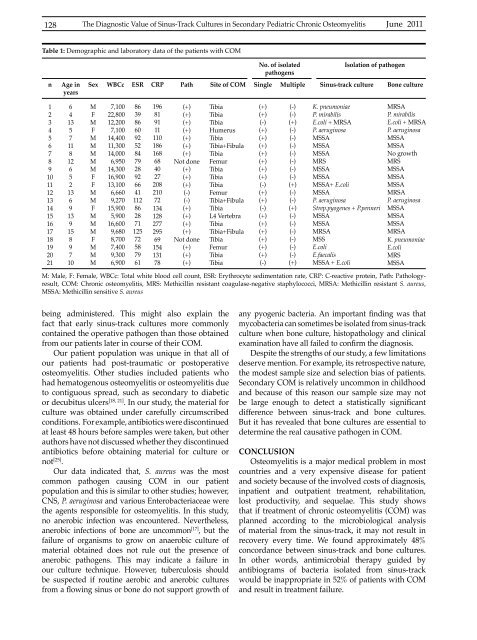
Table 1: Demographic and laboratory data of the patients with COM<br />
n<br />
Age in<br />
years<br />
No. of isolated<br />
pathogens<br />
Isolation of pathogen<br />
Sex WBCc ESR CRP Path Site of COM Single Multiple Sinus-track culture Bone culture<br />
1<br />
2<br />
3<br />
4<br />
5<br />
6<br />
7<br />
8<br />
9<br />
10<br />
11<br />
12<br />
13<br />
14<br />
15<br />
16<br />
17<br />
18<br />
19<br />
20<br />
21<br />
6<br />
4<br />
13<br />
5<br />
7<br />
11<br />
8<br />
12<br />
6<br />
5<br />
2<br />
13<br />
6<br />
9<br />
13<br />
9<br />
15<br />
8<br />
9<br />
7<br />
10<br />
M<br />
F<br />
M<br />
F<br />
M<br />
M<br />
M<br />
M<br />
M<br />
F<br />
F<br />
M<br />
M<br />
F<br />
M<br />
M<br />
M<br />
F<br />
M<br />
M<br />
M<br />
7,100<br />
22,800<br />
12,200<br />
7,100<br />
14,400<br />
11,300<br />
14,000<br />
6,950<br />
14,300<br />
16,900<br />
13,100<br />
6,660<br />
9,270<br />
15,900<br />
5,900<br />
16,600<br />
9,680<br />
8,700<br />
7,400<br />
9,300<br />
6,900<br />
86<br />
39<br />
86<br />
60<br />
92<br />
52<br />
84<br />
79<br />
28<br />
92<br />
66<br />
41<br />
112<br />
86<br />
28<br />
71<br />
125<br />
72<br />
58<br />
79<br />
61<br />
196<br />
81<br />
91<br />
11<br />
110<br />
186<br />
168<br />
68<br />
40<br />
27<br />
208<br />
210<br />
72<br />
134<br />
128<br />
277<br />
295<br />
69<br />
154<br />
131<br />
78<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
Not done<br />
(+)<br />
(+)<br />
(+)<br />
(-)<br />
(-)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
Not done<br />
(+)<br />
(+)<br />
(+)<br />
Tibia<br />
Tibia<br />
Tibia<br />
Humerus<br />
Tibia<br />
Tibia+Fibula<br />
Tibia<br />
Femur<br />
Tibia<br />
Tibia<br />
Tibia<br />
Femur<br />
Tibia+Fibula<br />
Tibia<br />
L4 Vertebra<br />
Tibia<br />
Tibia+Fibula<br />
Tibia<br />
Femur<br />
Tibia<br />
Tibia<br />
(+)<br />
(+)<br />
(-)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(-)<br />
(+)<br />
(+)<br />
(-)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(+)<br />
(-)<br />
(-)<br />
(-)<br />
(+)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(+)<br />
(-)<br />
(-)<br />
(+)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(-)<br />
(+)<br />
K. pneumoniae<br />
P. mirabilis<br />
E.coli + MRSA<br />
P. aeruginosa<br />
MSSA<br />
MSSA<br />
MSSA<br />
MRS<br />
MSSA<br />
MSSA<br />
MSSA+ E.coli<br />
MSSA<br />
P. aeruginosa<br />
Strep.pyogenes + P.penneri<br />
MSSA<br />
MSSA<br />
MRSA<br />
MSS<br />
E.coli<br />
E.faecalis<br />
MSSA + E.coli<br />
MRSA<br />
P. mirabilis<br />
E.coli + MRSA<br />
P. aeruginosa<br />
MSSA<br />
MSSA<br />
No growth<br />
MRS<br />
MSSA<br />
MSSA<br />
MSSA<br />
MRSA<br />
P. aeruginosa<br />
MSSA<br />
MSSA<br />
MSSA<br />
MRSA<br />
K. pneumoniae<br />
E.coli<br />
MRS<br />
MSSA<br />
M: Male, F: Female, WBCc: Total white blood cell count, ESR: Erythrocyte sedimentation rate, CRP: C-reactive protein, Path: Pathologyresult,<br />
COM: Chronic osteomyelitis, MRS: Methicillin resistant coagulase-negative staphylococci, MRSA: Methicillin resistant S. aureus,<br />
MSSA: Methicillin sensitive S. aureus<br />
being administered. This might also explain the<br />
fact that early sinus-track cultures more commonly<br />
contained the operative pathogen than those obtained<br />
from our patients later in course of their COM.<br />
Our patient population was unique in that all of<br />
our patients had post-traumatic or postoperative<br />
osteomyelitis. Other studies included patients who<br />
had hematogenous osteomyelitis or osteomyelitis due<br />
to contiguous spread, such as secondary to diabetic<br />
or decubitus ulcers [18, 21] . In our study, the material for<br />
culture was obtained under carefully circumscribed<br />
conditions. For example, antibiotics were discontinued<br />
at least 48 hours before samples were taken, but other<br />
authors have not discussed whether they discontinued<br />
antibiotics before obtaining material for culture or<br />
not [25] .<br />
Our data indicated that, S. aureus was the most<br />
common pathogen causing COM in our patient<br />
population and this is similar to other studies; however,<br />
CNS, P. aeruginosa and various Enterobacteriaceae were<br />
the agents responsible for osteomyelitis. In this study,<br />
no anerobic infection was encountered. Nevertheless,<br />
anerobic infections of bone are uncommon [17] , but the<br />
failure of <strong>org</strong>anisms to grow on anaerobic culture of<br />
material obtained does not rule out the presence of<br />
anerobic pathogens. This may indicate a failure in<br />
our culture technique. However, tuberculosis should<br />
be suspected if routine aerobic and anerobic cultures<br />
from a flowing sinus or bone do not support growth of<br />
any pyogenic bacteria. An important finding was that<br />
mycobacteria can sometimes be isolated from sinus-track<br />
culture when bone culture, histopathology and clinical<br />
examination have all failed to confirm the diagnosis.<br />
Despite the strengths of our study, a few limitations<br />
deserve mention. For example, its retrospective nature,<br />
the modest sample size and selection bias of patients.<br />
Secondary COM is relatively uncommon in childhood<br />
and because of this reason our sample size may not<br />
be large enough to detect a statistically significant<br />
difference between sinus-track and bone cultures.<br />
But it has revealed that bone cultures are essential to<br />
determine the real causative pathogen in COM.<br />
CONCLUSION<br />
Osteomyelitis is a major medical problem in most<br />
countries and a very expensive disease for patient<br />
and society because of the involved costs of diagnosis,<br />
inpatient and outpatient treatment, rehabilitation,<br />
lost productivity, and sequelae. This study shows<br />
that if treatment of chronic osteomyelitis (COM) was<br />
planned according to the microbiological analysis<br />
of material from the sinus-track, it may not result in<br />
recovery every time. We found approximately 48%<br />
concordance between sinus-track and bone cultures.<br />
In other words, antimicrobial therapy guided by<br />
antibiograms of bacteria isolated from sinus-track<br />
would be inappropriate in 52% of patients with COM<br />
and result in treatment failure.













