

Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw
Vol 43 # 2 June 2011 - Kma.org.kw

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>June</strong> <strong>2011</strong><br />
KUWAIT MEDICAL JOURNAL 141<br />
Fig. 5: Microscopic picture of the thyroid with papillary carcinoma<br />
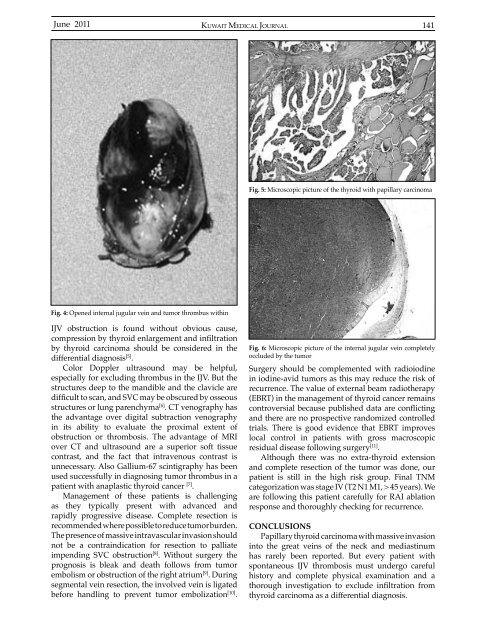
Fig. 4: Opened internal jugular vein and tumor thrombus within<br />
IJV obstruction is found without obvious cause,<br />
compression by thyroid enlargement and infiltration<br />
by thyroid carcinoma should be considered in the<br />
differential diagnosis [5] .<br />
Color Doppler ultrasound may be helpful,<br />
especially for excluding thrombus in the IJV. But the<br />
structures deep to the mandible and the clavicle are<br />
difficult to scan, and SVC may be obscured by osseous<br />
structures or lung parenchyma [6] . CT venography has<br />
the advantage over digital subtraction venography<br />
in its ability to evaluate the proximal extent of<br />
obstruction or thrombosis. The advantage of MRI<br />
over CT and ultrasound are a superior soft tissue<br />
contrast, and the fact that intravenous contrast is<br />
unnecessary. Also Gallium-67 scintigraphy has been<br />
used successfully in diagnosing tumor thrombus in a<br />
patient with anaplastic thyroid cancer [7] .<br />
Management of these patients is challenging<br />
as they typically present with advanced and<br />
rapidly progressive disease. Complete resection is<br />
recommended where possible to reduce tumor burden.<br />
The presence of massive intravascular invasion should<br />
not be a contraindication for resection to palliate<br />
impending SVC obstruction [8] . Without surgery the<br />
prognosis is bleak and death follows from tumor<br />
embolism or obstruction of the right atrium [9] . During<br />
segmental vein resection, the involved vein is ligated<br />
before handling to prevent tumor embolization [10] .<br />
Fig. 6: Microscopic picture of the internal jugular vein completely<br />
occluded by the tumor<br />
Surgery should be complemented with radioiodine<br />
in iodine-avid tumors as this may reduce the risk of<br />
recurrence. The value of external beam radiotherapy<br />
(EBRT) in the management of thyroid cancer remains<br />
controversial because published data are conflicting<br />
and there are no prospective randomized controlled<br />
trials. There is good evidence that EBRT improves<br />
local control in patients with gross macroscopic<br />
residual disease following surgery [11] .<br />
Although there was no extra-thyroid extension<br />
and complete resection of the tumor was done, our<br />
patient is still in the high risk group. Final TNM<br />
categorization was stage IV (T2 N1 M1, > 45 years). We<br />
are following this patient carefully for RAI ablation<br />
response and thoroughly checking for recurrence.<br />
CONCLUSIONS<br />
Papillary thyroid carcinoma with massive invasion<br />
into the great veins of the neck and mediastinum<br />
has rarely been reported. But every patient with<br />
spontaneous IJV thrombosis must undergo careful<br />
history and complete physical examination and a<br />
thorough investigation to exclude infiltration from<br />
thyroid carcinoma as a differential diagnosis.













