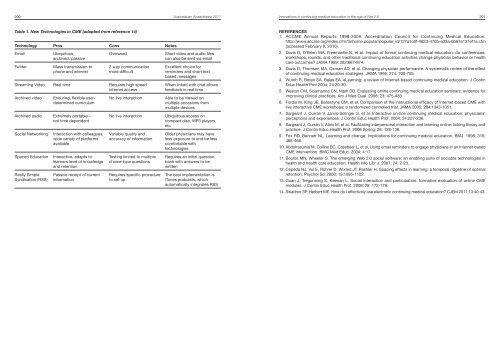
200 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Innovations in continuing medical education in the age of Net 2.0 201Table 1. <strong>New</strong> Technologies in CME (adapted from reference 14)Technology Pros Cons NotesEmailTwitterUbiquitous,archived, passiveMass transmission tophone <strong>and</strong> internetOverused2 way communicationmore difficultStreaming Video Real time Requires high speedinternet accessArchived videoEnduring, flexible userdeterminedcurriculumArchived audio Extremely portable –not time dependentSocial NetworkingSpaced EducationReally SimpleSyndication (RSS)Interaction with colleagues,wide variety of platformsavailableInteractive, adapts tolearners level of knowledge<strong>and</strong> retentionPassive receipt of currentinformationNo live interactionNo live interactionVariable quality <strong>and</strong>accuracy of informationTesting limited to multiplechoice-type questionsRequires specific procedureto set upShort video <strong>and</strong> audio filescan also be sent via emailExcellent choice forreminders <strong>and</strong> short textbased messagesWhen linked with chat allowsfeedback in real timeAble to be viewed onmultiple occasions frommultiple devicesUbiquitous access oncompact disc, MP3 players,etcOlder physicians may haveless exposure to <strong>and</strong> be lesscomfortable withtechnologiesRequires an initial questionbank with answers to bewrittenThe best implementation isiTunes podcasts, whichautomatically integrates RSSREFERENCES1. ACCME Annual Reports 1998-2009. Accreditation Council for Continuing Medical Education.http://www.accme.org/index.cfm/fa/home.popular/popular_id/127a1c6f-462d-476b-a33a-6b67e131ef1a.cfm(accessed February 9, 2010).2. Davis D, O’Brien MA, Freemantle N, et al. Impact of formal continuing medical education: do conferences,workshops, rounds, <strong>and</strong> other traditional continuing education activities change physician behavior or healthcare outcomes? JAMA 1999; 282:867-874.3. Davis D, Thomson MA, Oxman AD, et al. Changing physician performance. A systematic review of the effectof continuing medical education strategies. JAMA 1995; 274: 700-705.4. Wutoh R, Boren SA, Balas EA. eLearning: a review of Internet-based continuing medical education. J ContinEduc Health Prof 2004; 24:20-30.5. Weston CM, Sciamanna CN, Nash DB. Evaluating online continuing medical education seminars: evidence forimproving clinical practices. Am J Med Qual. 2008; 23: 475-483.6. Fordis M, King JE, Ballantyne CM, et al. Comparison of the instructional efficacy of Internet-based CME withlive interactive CME workshops: a r<strong>and</strong>omized controlled trial. JAMA 2005; 294:1043-1051.7. Sargeant J, Curran V, Jarvis-Selinger S, et al. Interactive on-line continuing medical education: physicians’perceptions <strong>and</strong> experiences. J Contin Educ Health Prof. 2004; 24:227-236.8. Sargeant J, Curran V, Allen M, et al. Facilitating interpersonal interaction <strong>and</strong> learning online: linking theory <strong>and</strong>practice. J Contin Educ Health Prof. 2006 Spring; 26: 128-136.9. Fox RD, Bennett NL. Learning <strong>and</strong> change: implications for continuing medical education. BMJ. 1998; 316:466-468.10. Abdolrasulnia M, Collins BC, Casebeer L, et al. Using email reminders to engage physicians in an Internet-basedCME intervention. BMC Med Educ. 2004; 4:17.11. Boulos MN, Wheeler S. The emerging Web 2.0 social software: an enabling suite of sociable technologies inhealth <strong>and</strong> health care education. Health Info Libr J. 2007; 24: 2-23.12. Cepeda NJ, Vul E, Rohrer D, Wixted JT, Pashler H. Spacing effects in learning: a temporal ridgeline of optimalretention. Psychol Sci 2008; 19:1095-1102.13. Guan J, Tregonning S, Keenan L. Social interaction <strong>and</strong> participation: formative evaluation of online CMEmodules. J Contin Educ Health Prof. 2008; 28 :172-179.14. Swadron SP, Herbert ME. How do I effectively use electronic continuing medical education? CJEM <strong>2011</strong>;13:40-43.
What next for anaesthesia in Australia? 203What next for anaesthesia in Australia?DR RICHARD HALLIWELL. MB BS, FANZCA. ANAESTHETIST, WESTMEAD HOSPITAL, SYDNEY, NSW.Dr Halliwell is a Senior Staff Specialist Anaesthetist at Westmead Hospital, <strong>and</strong> Clinical Senior Lecturer, Disciplineof <strong>Anaesthesia</strong>, Sydney Medical School, University of Sydney. He holds several committee positions in <strong>Anaesthesia</strong>,Medicine, <strong>and</strong> Clinical Pharmacology. He has a particular interest in clinical trials.INTRODUCTIONIt has been said we can only see the future ‘…through a glass darkly’. Predicting the future is fraught with danger.History is littered with predications that now seem ludicrous. Some curious examples include the following;“Everything that can be invented has been invented” (official of the US Patent Office, 1899). More closely relatedto medicine, from one who would be expected to know better, “We can close the books on infectious diseases”(William H. Stewart, US Surgeon General, 1969). Despite these epic fails, I will venture to make predictions aboutthe future of anaesthesia in Australia.RECENT HISTORYIn 1986, as a registrar, I thought anaesthesia had reached a state of refinement <strong>and</strong> maturity, <strong>and</strong> that furtherprogress seemed unlikely or even unnecessary. Drugs such as thiopentone <strong>and</strong> isoflurane worked well <strong>and</strong> fairlysafely. Injections of pethidine, if really necessary, were the rule for pain relief; any review of pain relief was delegatedto an intern. Patients were admitted a day or two before surgery for leisurely review, <strong>and</strong> they did not leave hospitaluntil after many days (or weeks) of recuperation. The marvels of technology meant patients had their ECG monitoredroutinely <strong>and</strong> new machines could measure the blood pressure automatically. Then it seemed that nothing elsemore could be imagined to improve the practice of anaesthesia. With hindsight, that view of mature practice wasproven completely wrong. I wonder how anaesthetists in 20 years time will look back <strong>and</strong> consider today’s practiceof anaesthesia.ANAESTHESIA PROVIDERSA substantial issue facing the specialty of anaesthesia is alternative providers, such as nurse anaesthetists. Thishas been on the public agenda for several decades <strong>and</strong> does not appear to have been resolved in the public’smind. 1,2,3 Other providers are seen as a realistic alternative to specialist anaesthetists. The public <strong>and</strong> insurers seethis as a legitimate way of containing healthcare expenditure <strong>and</strong> solving the shortage of anaesthetists. This remainsa real threat while anaesthetists stay focused on the procedural <strong>and</strong> technical aspects of their practice <strong>and</strong> not thebroader medical skills we can bring to the surgical patient. Unfortunately, anaesthesia has become so safe, thatthe public, politicians <strong>and</strong> insurers perceive it as unsophisticated, straightforward <strong>and</strong> routine. Many members ofthe public do not know that anaesthetists are medical doctors <strong>and</strong> think we are technicians or paramedics.PROGRESS IN ANAESTHESIAWhat is needed is the development of anaesthesia to progress to a higher level. This should include the embracingof perioperative medicine. Anaesthetists are uniquely placed, compared with other specialties, to expertly undertakethis important area of care. This approach has already been shown to significantly reduce postoperative mortalityin an <strong>Australian</strong> teaching hospital. 4 This role will build the profile of anaesthetists in the eye of patients, their relatives<strong>and</strong> our medical colleagues. It will take us out of the hidden realm of the operating theatre. We will develop apositive, close relationship with our patients. We will not just be seen as the mysterious person that appears momentsbefore the patient fades into unconsciousness.Why do patients vary so much in their response to drugs? Some variation can be explained by patient’s age,underlying physiology or drug tolerance. However, seemingly similar patients can still be markedly different in theirresponse <strong>and</strong> dose requirements. <strong>New</strong> developments in phamacogenetics can explain these puzzling individualdifferences. Some of our commonly used drugs are subject to this effect. For example, codeine is a drug whoseresponse is strongly influenced by genetics. Codeine itself is just a prodrug. It depends on conversion to morphineto have its analgesic effect. This enzymatic conversion is dependent on CYP2D6 activity which is significantlyvariable. The activity of CYP2D6 can be tested in patients prospectively. This approach shows the ability to tailordrug selection based on an individual patient’s genetic profile. Other drugs that are known to be influenced byindividual pharmacogenetics include ondansetron, warfarin, clopidogrel <strong>and</strong> tramadol. The future holds the possibilityof testing patients pharmacogenetic makeup <strong>and</strong> using this knowledge to avoid drugs that may be either ineffectiveor cause significant toxicity.What makes a profession different from an occupation? What makes us different from the competent builder,the plumber or the mechanic, with whom we have a good <strong>and</strong> personal relationship? A profession not only deliversa product, it also develops the product through research. This important distinction, that sets anaesthetists apartfrom alternative providers, is the professional activity of advancing the body of knowledge through research.Research is important to not only improve the st<strong>and</strong>ard of care for patients but also to demonstrate to the public,who have an interest in medical research, that we can make important improvements to the care of patients. InAustralia, there have been prominent achievements in anaesthesia research through the activities of the ANZCAClinical Trials Group which has been successful in publishing research in high-impact medical journals (for exampleENIGMA, POISE, MASTER, B-AWARE). These have gripped the public’s attention <strong>and</strong> have featured prominently