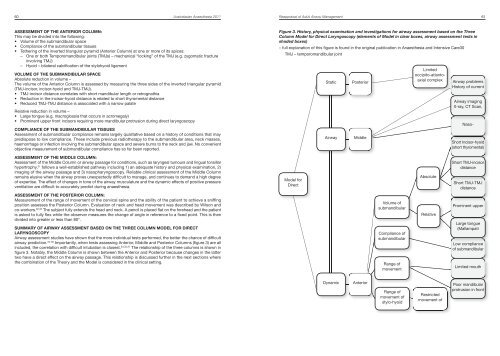
60 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Reappraisal of Adult Airway Management 61ASSESSMENT OF THE ANTERIOR COLUMN:This may be divided into the following:• Volume of the subm<strong>and</strong>ibular space• Compliance of the subm<strong>and</strong>ibular tissues• Tethering of the inverted triangular pyramid (Anterior Column) at one or more of its apices:– One or both Temporom<strong>and</strong>ibular joints (TMJs) – mechanical “locking” of the TMJ (e.g. zygomatic fractureinvolving TMJ)– Hyoid – bilateral calcification of the stylohyoid ligamentVOLUME OF THE SUBMANDIBULAR SPACEAbsolute reduction in volume –The volume of the Anterior Column is assessed by measuring the three sides of the inverted triangular pyramid(TMJ-incisor, incisor-hyoid <strong>and</strong> TMJ-TMJ).• TMJ-incisor distance correlates with short m<strong>and</strong>ibular length or retrognathia• Reduction in the incisor-hyoid distance is related to short thyromental distance• Reduced TMJ-TMJ distance is associated with a narrow palateRelative reduction in volume –• Large tongue (e.g. macroglossia that occurs in acromegaly)• Prominent upper front incisors requiring more m<strong>and</strong>ibular protrusion during direct laryngoscopyCOMPLIANCE OF THE SUBMANDIBULAR TISSUESAssessment of subm<strong>and</strong>ibular compliance remains largely qualitative based on a history of conditions that maypredispose to low compliance. These include previous radiotherapy to the subm<strong>and</strong>ibular area, neck masses,haemorrhage or infection involving the subm<strong>and</strong>ibular space <strong>and</strong> severe burns to the neck <strong>and</strong> jaw. No convenientobjective measurement of subm<strong>and</strong>ibular compliance has so far been reported.Figure 3. History, physical examination <strong>and</strong> investigations for airway assessment based on the ThreeColumn Model for Direct Laryngoscopy (elements of Model in clear boxes, airway assessment tests inshaded boxes)– full explanation of this figure is found in the original publication in <strong>Anaesthesia</strong> <strong>and</strong> Intensive Care30TMJ – temporom<strong>and</strong>ibular jointStaticAirwayPosteriorMiddleLimitedoccipito-atlantoaxialcomplexAirway problemsHistory of currentAirway imagingX-ray, CT Scan,Naso-Short Incisor-hyoid(short thyromental)ASSESSMENT OF THE MIDDLE COLUMN:Assessment of the Middle Column or airway passage for conditions, such as laryngeal tumours <strong>and</strong> lingual tonsillarhypertrophy, 31 follows a well-established pathway including 1) an adequate history <strong>and</strong> physical examination, 2)imaging of the airway passage <strong>and</strong> 3) nasopharyngoscopy. Reliable clinical assessment of the Middle Columnremains elusive when the airway proves unexpectedly difficult to manage, <strong>and</strong> continues to dem<strong>and</strong> a high degreeof expertise. The effect of changes in tone of the airway musculature <strong>and</strong> the dynamic effects of positive pressureventilation are difficult to accurately predict during anaesthesia.Model forDirectAbsoluteShort TMJ-incisordistanceShort TMJ-TMJdistanceASSESSMENT OF THE POSTERIOR COLUMN:Measurement of the range of movement of the cervical spine <strong>and</strong> the ability of the patient to achieve a sniffingposition assesses the Posterior Column. Evaluation of neck <strong>and</strong> head movement was described by Wilson <strong>and</strong>co-workers. 32,33 The subject fully extends the head <strong>and</strong> neck. A pencil is placed flat on the forehead <strong>and</strong> the patientis asked to fully flex while the observer measures the change of angle in reference to a fixed point. This is thendivided into greater or less than 80°.SUMMARY OF AIRWAY ASSESSMENT BASED ON THE THREE COLUMN MODEL FOR DIRECTLARYNGOSCOPYAirway assessment studies have shown that the more individual tests performed, the better the chance of difficultairway prediction. 34-36 Importantly, when tests assessing Anterior, Middle <strong>and</strong> Posterior Columns (figure 3) are allincluded, the correlation with difficult intubation is closest. 34,35,37 The relationship of the three columns is shown infigure 3. Notably, the Middle Column is shown between the Anterior <strong>and</strong> Posterior because changes in the lattertwo have a direct effect on the airway passage. This relationship is discussed further in the next sections wherethe combination of the Theory <strong>and</strong> the Model is considered in the clinical setting.Volume ofsubm<strong>and</strong>ibularCompliance ofsubm<strong>and</strong>ibularRange ofmovementRelativeProminent upperLarge tongue(MallampatiLow complianceof subm<strong>and</strong>ibularLimited mouthDynamicAnteriorRange ofmovement ofstylo-hyoidRestrictedmovement ofPoor m<strong>and</strong>ibularprotrusion in front
62 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Reappraisal of Adult Airway Management 63COMBINING THE TWO-CURVE THEORY AND THREE COLUMN MODELFigure 4 shows how both the Anterior <strong>and</strong> Posterior Columns of the Three Column Model for Direct Laryngoscopyinfluence the airway passage (Middle Column) configuration, that is the Two-Curves. Changes in the PosteriorColumn have a direct effect on the Primary <strong>and</strong> Secondary Curves – extension: flattening Primary Curve, head lift:flattening Secondary Curve.In contrast, the effect of the Anterior Column on the Primary <strong>and</strong> Secondary Curves is the result of both pathologyof the column <strong>and</strong> the impact different airway devices have on it. For instance, variations in the Anterior Columnthat occur in retrognathia <strong>and</strong> macroglossia will affect the shape of the airway curves. In addition, the effect ofairway devices on the curves may vary from little or none in the case of fibreoptic bronchoscopy <strong>and</strong> Glidescopevideolaryngoscope TM to marked flattening of the Primary Curve with the C-Mac video laryngoscope TM .Finally, intrinsic lesions of the airway passage (or Middle Column), such as foreign bodies <strong>and</strong> airway tumours,may distort the Primary <strong>and</strong> Secondary Curves.Figure 4. Both the anterior (triangle) <strong>and</strong> posterior (black line) columns of the Model for DirectLaryngoscopy influence the shape of the airway passage configuration (black dotted line) as describedin the Two-Curve Theory.EXAMPLES OF AIRWAY MANAGEMENT BASED ON THE TWO-CURVES THEORY AND THE THREECOLUMN MODELAnterior Column ProblemsAnterior Column problems are a diverse group of pathological conditions which may be divided into (i) reducedvolume of the subm<strong>and</strong>ibular space (retrognathia/micrognathia), (ii) reduced compliance of the subm<strong>and</strong>ibulartissues (including Ludwig’s angina, post-radiotherapy to the subm<strong>and</strong>ibular space <strong>and</strong> tumour of the tongue base)<strong>and</strong> (iii) restriction of temporo-m<strong>and</strong>ibular joint function.Optimising head <strong>and</strong> neck position is essential to ensure flattening of the Secondary Curve before focusing onthe Primary Curve with Anterior Column problems. With reduced volume or reduced compliance of the subm<strong>and</strong>ibularspace, the Primary Curve is the major focus of management. There are two potential management plans for dealingwith Primary Curve problems.1) Paraglossal or retromolar insertion of a straight laryngoscope:Magill described a technique later called by Bonfil 38 “homolateral retromolar intubation” which allows the operatorto bypass the Primary Curve <strong>and</strong> enter the supraglottic space (rostral part of Secondary Curve). Henderson 39,40re-visited this concept, using a low profile straight blade with a paraglossal approach rather than the midline for apatient with a hypoplastic m<strong>and</strong>ible 40,41 <strong>and</strong> limited forward movement of the hyoid. 402) Following the Primary Curve without displacing the subm<strong>and</strong>ibular tissues:Methods that manoeuvre around the Primary Curve without causing its displacement include flexible fibreopticbronchoscopy, rigid indirect laryngoscopy devices <strong>and</strong> blind nasal intubation. Successful use of the GlideScopevideolaryngoscope TM has been described for tracheal intubation of patients with m<strong>and</strong>ibular hypoplasia. 42,43 Blindintubation techniques including blind nasal intubation 44 <strong>and</strong> lightw<strong>and</strong>s such as the Trachlight TM have been usedfor m<strong>and</strong>ibular hypoplasia 45-47 <strong>and</strong> patients with limited mouth opening. 47,48The choice should be based on the experience of the operator <strong>and</strong> the suitability of the available device ortechnique.POSTERIOR COLUMN PROBLEMSElective patients with normal Anterior Column requiring manual in-line neck stabilisation (MILNS):The levered laryngoscope when activated produces a fulcrum at the base of the tongue, which increases pressureon the hyo-epiglottic ligament. This elevates the epiglottis in patients with normal Anterior Columns <strong>and</strong> flattensboth the Primary <strong>and</strong> importantly, the Secondary Curve. The levered blade has been used successfully in at leastthree studies examining its role in patients requiring manual in-line stabilisation of the neck or wearing cervicalcollars49-51 where the Anterior Column is normal.CLINICAL CONDITIONS WITH COMBINED ANTERIOR, MIDDLE AND POSTERIOR COLUMN PROBLEMSAcromegaly:Features of acromegaly that may cause difficult laryngoscopy <strong>and</strong> intubation 52 include macroglossia, prognathism,cervical spine osteophyte formation with decreased range of movement, thickening of the pharyngo-laryngeal softtissues <strong>and</strong> recurrent laryngeal nerve palsy. The problems are three-fold. Firstly, there is inability to compress theenlarged swollen tongue (Anterior Column) during direct laryngoscopy despite the increased subm<strong>and</strong>ibular volumecreated by the prognathism. Secondly, there is encroachment into the airway passage by swollen upper airwaymucosa (Middle Column). Lastly, restricted neck mobility may interfere with positioning in the sniffing position.Though all patients may not exhibit all of these aspects, they do have a potential for problems with all three columns.If there is no osteophyte formation <strong>and</strong> the difficulty is mainly due to the Anterior Column, then a straightlaryngoscope blade used in conjunction with a curved-tip bougie may be effective in displacing the enlarged tongue.An airway passage restricted by thickened or redundant mucosa may, however, make the narrower straight bladeless effective. It seems that an indirect laryngoscopy device, intubating laryngeal mask or fibreoptic bronchoscopyshould be more reliable, but mixed results have been found with indirect laryngoscopy devices. The intubatinglaryngeal mask has a 47.4% failure rate. 53 This appears to be related to the difficulty in matching the Primary Curveof acromegalics to the fixed curvature of a device that has an integral tracheal tube conduit. Preliminary reports 52indicate that use of a flexible bronchoscope through a Classic LMA TM may provide flexibility to match the patient’sPrimary Curvature. The GlideScope videolaryngoscope TM separates the device from the tube/stylet <strong>and</strong> allows foreasier manoeuvrability in the airway with high success. 52Awake fibreoptic intubation 54-56 provides a useful alternative to indirect laryngoscopy methods, especially if allthree aspects of the model are involved.CONCLUSIONIn Eugene Wigner’s “The Unreasonable Effectiveness of Mathematics in the Natural Sciences”, he states that themathematical structure of physics often leads to further advances in theory <strong>and</strong> even empirical predictions. This isa significant statement. They are interwoven <strong>and</strong>, despite their complexities, predictable. We need a similarmathematical model for airway management that will explain what we know <strong>and</strong> will predict what we should cometo underst<strong>and</strong>.The Two-Curve Theory <strong>and</strong> the Three Column Model of Direct Laryngoscopy provide a basis for teaching <strong>and</strong>ongoing research in this area. The foundation stone of this approach is assessment of the airway. This may beeither embarking on airway management or as an urgent reappraisal when an unexpected difficult airway isencountered. The diagnosis will assist the operator to select an airway manoeuvre that is likely to be successful<strong>and</strong> to avoid those that are not.These two theories are based partly on experimental work <strong>and</strong> partly on “scholastic reasoning”. With time theymay remain unchanged, be modified or need replacing.“Imagination is more important than knowledge. Knowledge is limited; imagination encircles the world.”~ Albert Einstein