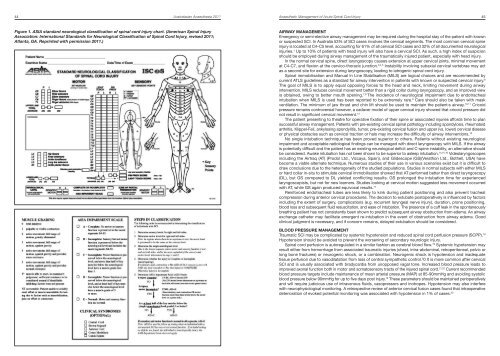
44 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Anaesthetic Management of Acute Spinal Cord Injury 45Figure 1. ASIA st<strong>and</strong>ard neurological classification of spinal cord injury chart. (American Spinal InjuryAssociation: International St<strong>and</strong>ards for Neurological Classification of Spinal Cord Injury, revised <strong>2011</strong>;Atlanta, GA. Reprinted with permission <strong>2011</strong>.)AIRWAY MANAGEMENTEmergency or semi-elective airway management may be required during the hospital stay of the patient with knownor suspected SCI. In Australia 53% of SCI cases involves the cervical segments. The most common cervical spineinjury is located at C4–C5 level, accounting for 61% of all cervical SCI cases <strong>and</strong> 32% of all documented neurologicalinjuries. 1 Up to 10% of patients with head injury will also have a cervical SCI. As such, a high index of suspicionshould be employed during airway management of the traumatically injured patient, especially with head injury.In the normal cervical spine, direct laryngoscopy causes extension at upper cervical joints, minimal movementat C4-C7, <strong>and</strong> flexion at the cervico-thoracic junction. 3,4,5 Instability involving subaxial cervical vertebrae may actas a second site for extension during laryngoscopy, leading to iatrogenic spinal cord injury.Spinal immobilisation <strong>and</strong> Manual In Line Stabilisation (MILS) are logical choices <strong>and</strong> are recommended bycurrent ATLS guidelines as a st<strong>and</strong>ard for airway intervention in patients with known or suspected cervical injury. 6The goal of MILS is to apply equal opposing forces to the head <strong>and</strong> neck, limiting movement during airwayintervention. MILS reduces cervical movement better than a rigid collar during laryngoscopy, <strong>and</strong> an improved viewis obtained, owing to better mouth opening. 7,8 The incidence of neurological impairment due to endotrachealintubation when MILS is used has been reported to be extremely rare. 9 Care should also be taken with maskventilation. The minimum of jaw thrust <strong>and</strong> chin lift should be used to maintain the patient›s airway. 10,11 Cricoidpressure remains controversial however, a cadaver model of upper cervical injury showed that cricoid pressure didnot result in significant cervical movement. 12The patient presenting to theatre for operative fixation of their spine or associated injuries affords time to plansuccessful airway management. Patients with pre-existing cervical spinal pathology including spondylosis, rheumatoidarthritis, Klippel-Feil, ankylosing spondylitis, tumor, pre-existing cervical fusion <strong>and</strong> upper (vs. lower) cervical diseaseor physical obstacles such as cervical traction or halo may increase the difficulty of airway interventions. 13No single intubation technique has been proved superior to others. Patients without existing neurologicalimpairment <strong>and</strong> acceptable radiological findings can be managed with direct laryngoscopy with MILS. If the airwayis potentially difficult <strong>and</strong> the patient has an existing neurological deficit <strong>and</strong> C-spine instability, an alternative shouldbe considered. Awake intubation has not been shown to be superior to asleep intubation. 14,15,16 Videolaryngoscopesincluding the Airtraq (AT) (Prodol Ltd., Vizcaya, Spain), <strong>and</strong> Glidescope (GS)(Verathon Ltd., Bothell, USA) havebecome a viable alternate technique. Numerous studies of their use in various scenarios exist but it is difficult todraw conclusions due to the heterogeneity of the studied populations. Studies in normal subjects with either MILSor hard collar in-situ to stimulate cervical immobilisation showed that AT performed better than direct laryngoscopy(DL), but GS compared to DL yielded conflicting results. GS prolonged the intubation time for experiencedlaryngoscopists, but not for new learners. Studies looking at cervical motion suggested less movement occurredwith AT, while GS again produced equivocal results. 17Reinforced endotracheal tubes are less likely to kink during patient positioning <strong>and</strong> also prevent trachealcompression during anterior cervical procedures. The decision to extubate postoperatively is influenced by factorsincluding the extent of surgery, complications (e.g. recurrent laryngeal nerve injury), duration, prone positioning,blood loss <strong>and</strong> subsequent fluid resuscitation, <strong>and</strong> ease of intubation. The presence of a cuff leak in the spontaneouslybreathing patient has not consistently been shown to predict subsequent airway obstruction from edema. An airwayexchange catheter may facilitate emergent re-intubation in the event of obstruction from airway edema. Goodclinical judgment is necessary, <strong>and</strong> if concern remains, delayed extubation should be considered.BLOOD PRESSURE MANAGEMENTTraumatic SCI may be complicated by systemic hypotension <strong>and</strong> reduced spinal cord perfusion pressure (SCPP). 18Hypotension should be avoided to prevent the worsening of secondary neurologic injury.Spinal cord perfusion is autoregulated in a similar fashion as cerebral blood flow. 19 Systemic hypotension mayresult either from hemorrhage from associated traumatic injuries (chest, intra-abdominal, retroperitoneal, pelvic orlong bone fractures) or neurogenic shock, or a combination. Neurogenic shock is hypotension <strong>and</strong> inadequatetissue perfusion due to vasodilatation from loss of central sympathetic control. 2 0 It is more common after cervicalSCI <strong>and</strong> is usually associated with bradycardia from unopposed vagal tone. Increased blood pressure leads toimproved axonal function both in motor <strong>and</strong> somatosensory tracts of the injured spinal cord. 21,22 Current recommendedblood pressure targets include maintenance of mean arterial pressure (MAP) at 85-90mmHg <strong>and</strong> avoiding systolicblood pressure below 90mmHg for up to five days post injury. 18 These parameters should be maintained perioperatively<strong>and</strong> will require judicious use of intravenous fluids, vasopressors <strong>and</strong> inotropes. Hypotension may also interferewith neurophysiological monitoring. A retrospective review of anterior cervical fusion cases found that intraoperativedeterioration of evoked potential monitoring was associated with hypotension in 1% of cases. 23
46 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Anaesthetic Management of Acute Spinal Cord Injury 47FLUID MANAGEMENTSeveral strategies have been used to minimize intraoperative blood loss. Elevation of the intra-abdominal pressureshould be avoided. An operative table with the Jackson frame attachment is preferable, enabling the abdomen tohang free. This reduces epidural venous bleeding when compared to positioning prone on the Wilson frame. 24Antifibrinolytic agents have been shown to decrease intraoperative <strong>and</strong> total perioperative blood loss in patientsundergoing spinal fusion. A r<strong>and</strong>omised study showed an absolute but non-significant decrease in both totalperioperative blood loss <strong>and</strong> transfusion requirements using aminocaproic acid compared to control. 25 A r<strong>and</strong>omisedstudy of tranexamic acid versus placebo for spinal fusions showed significantly less perioperative blood losscompared to placebo, but no difference in the amount of blood products transfused between the two groups. 26There was no increase in thromboembolic complications.A small r<strong>and</strong>omised dose escalation trial using recombinant factor VIIa (rFVIIa) in spinal fusion showed anabsolute but non significant decrease in intraoperative blood loss for the rFVIIa groups at any dose studied. 27 Onethromboembolic event causing death was reported in the rFVIIa group.Studies reporting the effectiveness of cell saver in reducing the need for homologous transfusion have shownvariable results. A recent systematic review of cell saver in routine elective spine surgery concluded that there isinsufficient evidence in the literature to support its cost-effective use. 28Optimal fluid therapy in SCI patients remains unknown. Hypotonic crystalloids such as 5% dextrose <strong>and</strong> 0.45%normal saline however, may exacerbate cord swelling <strong>and</strong> should be avoided. Albumin use is contraindicated inpatients with concurrent traumatic brain injury following report of increased mortality from the SAFE-TBI study. 29,30EVOKED POTENTIAL MONITORINGModern intraoperative neurological monitoring during spinal surgery includes evoked potential monitoring (sensory<strong>and</strong> motor) <strong>and</strong> spontaneous electromyography (EMG).Somatosensory evoked potentials (SSEP) are elicited by stimulation over peripheral nerves <strong>and</strong> recordingresponses at some point along the sensory pathway, usually the somatosensory cortex. Motor evoked potential(MEP) monitoring involves transcortical stimulation over the motor cortex <strong>and</strong> recording the muscle response. EMGcan detect nerve root irritation by electrode placement in the innervated muscle group.The aim of evoked potential monitoring is the early detection of worsening spinal cord function, giving theopportunity to correct offending factors such as: patient position (e.g. neck position, shoulder position), hypotension,hypothermia, <strong>and</strong> factors related to the surgical intervention. A recent systematic review indicated that there is onlylow level evidence that intraoperative neuromonitoring reduces the rate of new or worsening neurologic deficits. 31Total intravenous anaesthesia (TIVA) without muscle relaxation is required for MEP monitoring. Volatile anesthetics<strong>and</strong> nitrous oxide are best avoided as they cause a dose-dependent reduction in MEP signal amplitude, commencingat low concentrations.Volatiles suppress cortical SSEPs in a dose dependant way, especially above 0.5 MAC. TIVA provides bettermonitoring conditions. Volatile anesthetics may also be used for spontaneous EMG recording, provided musclerelaxants are avoided. Opioids do not impact evoked potential monitoring <strong>and</strong> ketamine has been shown to enhanceevoked potential monitoring. 32 Dexmedetomidine has been used as a supplement to TIVA, without detriment toevoked potential monitoring. 33,34 A stable anesthesia without significant changes in blood pressure or dosing ofanesthetic agents needs to be provided so that changes in evoked responses may be attributed solely to surgicaltechnique.CONCLUSIONThe anaesthetist plays a crucial role in the perioperative management of patients with spinal cord injury. The overallgoal of anaesthetic management is the prevention of secondary injury to the spinal cord. This paper presentsan overview to the assessment, <strong>and</strong> summarises evidence for successful anaesthetic management of thecord-injured patient.REFERENCES1. Norton L. Spinal cord injury Australia 2007-2008. <strong>Australian</strong> Institute of Health <strong>and</strong> Welfare. 2010. p. 13,18.2. Association ASI. Reference Manual of the International St<strong>and</strong>ards for Neurological Classification of Spinal CordInjury. American Spinal Injury Association 2003.3. Lennarson PJ, Smith DW, Sawin PD, Todd MM, Sato Y, Traynelis VC. Cervical spinal motion during intubation:Efficacy of stabilization maneuvers in the setting of complete segmental instability. J Neurosurg 2001;94:265-70.4. Lennarson PJ, Smith D, Todd MM, Carras D, Sawin PD, Brayton J, et al. Segmental cervical spine motionduring orotracheal intubation of the intact <strong>and</strong> injured spine with <strong>and</strong> without external stabilization. J Neurosurg2000;92:201-6.5. Sawin PD, Todd MM, Traynelis VC, Farrell SB, Nader A, Sato Y, et al. Cervical spine motion with directlaryngoscopy <strong>and</strong> orotracheal intubation. An in vivo cinefluoroscopic study of subjects without cervicalabnormality. Anesthesiology 1996;85:26-36.6. American College of Surgeons CoT. Advanced Trauma Life Support Student Course Manual. Advanced TraumaLife Support Student Course Manual, 8 th ed. Chicago; 2008. p. 168.7. Heath KJ. The effect of laryngoscopy of different cervical spine immobilisation techniques. <strong>Anaesthesia</strong>1994;49:843-5.8. Aoi Y, Inagawa G, Hashimoto K, Tashima H, Tsuboi S, Takahata T, et al. Airway Scope Laryngoscopy UnderManual Inline Stabilization <strong>and</strong> Cervical Collar Immobilization: A Crossover In Vivo Cinefluoroscopic Study.J Trauma 2010.9. Manoach S, Paladino L. Manual in-line stabilization for acute airway management of suspected cervical spineinjury: Historical review <strong>and</strong> current questions. Ann Emerg Med 2007;50:236-45.10. Aprahamian C, Thompson BM, Finger WA, Darin JC. Experimental cervical spine injury model: Evaluationof airway management <strong>and</strong> splinting techniques. Ann Emerg Med 1984;13:584-7.11. Hauswald M, Sklar DP, T<strong>and</strong>berg D, Garcia JF. Cervical spine movement during airway management:Cinefluoroscopic appraisal in human cadavers. Am J Emerg Med 1991;9:535-538.12. Donaldson WF 3 rd, Heil BV, Donaldson VP, Silvaggio VJ. The effect of airway maneuvers on the unstableC1-C2 segment. A cadaver study. Spine (Phila Pa 1976) 1997;22:1215-8.13. Calder I, Calder J, Crockard HA. Difficult direct laryngoscopy in patients with cervical spine disease. <strong>Anaesthesia</strong>1995;50:756-63.14. Popitz MD. Anesthetic implications of chronic disease of the cervical spine. Anesth Analg 1997;84:672-83.15. Crosby ET, Lui A. The adult cervical spine: Implications for airway management. Can J Anaesth 1990;37:77-93.16. Suderman VS, Crosby ET, Lui A. Elective oral tracheal intubation in cervical spine-injured adults. Can J Anaesth1991;38:785-9.17. Cheyne D, Doyle P. Advances in laryngoscopy: rigid indirect laryngoscopy. F1000 Med Reports 2010, 2:6118. AANS/CNS. Blood Pressure Management after Acute Spinal Cord Injury. Neurosurgery 2002;50:S58-S62.19. Kobrine AI, Doyle TF, Rizzoli HV. Spinal cord blood flow as affected by changes in systemic arterial bloodpressure. J Neurosurg 1976;44:12-5.20. Wuermser LA, Ho CH, Chiodo AE, Priebe MM, Kirshblum SC, Scelza WM. Spinal cord injury medicine. 2. Acutecare management of traumatic <strong>and</strong> nontraumatic injury. Arch Phys Med Rehabil 2007;88:S55-61.21. Ploumis A, Yadlapalli N, Fehlings MG, Kwon BK, Vaccaro AR. A systematic review of the evidence supportinga role for vasopressor support in acute SCI. Spinal Cord 2010;48:356-62.22. King BS, Gupta R, Narayan RK. The early assessment <strong>and</strong> intensive care unit management of patients withsevere traumatic brain <strong>and</strong> spinal cord injuries. Surg Clin North Am 2000;80:855-70.23. Lee JY, Hilibr<strong>and</strong> AS, Lim MR, Zavatsky J, Zeiller S, Schwartz DM, et al. Characterization of neurophysiologicalerts during anterior cervical spine surgery. Spine (Phila Pa 1976) 2006;31:1916-22.24. Bess RS, Lenke LG. Blood loss minimization <strong>and</strong> blood salvage techniques for complex spinal surgery. NeurosurgClin N Am 2006;17:227-34.25. Urban MK, Beckman J, Gordon M, Urquhart B, Boachie-Adjei O. The efficacy of antifibrinolytics in the reductionof blood loss during complex adult reconstructive spine surgery. Spine (Phila Pa 1976) 2001;26:1152-6.26. Wong J, El Beheiry H, Rampersaud YR, Lewis S, Ahn H, De Silva Y, et al. Tranexamic Acid reduces perioperativeblood loss in adult patients having spinal fusion surgery. Anesth Analg 2008;107:1479-86.27. Sachs B, Delacy D, Green J, Graham RS, Ramsay J, Kreisler N, et al. Recombinant activated factor VII in spinalsurgery: A multicenter, r<strong>and</strong>omized, double-blind, placebo-controlled, dose-escalation trial. Spine (Phila Pa1976) 2007;32:2285-93.28. Elgafy H, Bransford RJ, McGuire RA, Dettori JR, Fischer D. Blood loss in major spine surgery: Are there effectivemeasures to decrease massive hemorrhage in major spine fusion surgery? Spine (Phila Pa 1976) 2010;35:S47-56.29. Finfer S, Bellomo R, Boyce N, French J, Myburgh J, Norton R. A comparison of albumin <strong>and</strong> saline for fluidresuscitation in the intensive care unit. N Engl J Med 2004;350:2247-56.30. Choi PT, Yip G, Quinonez LG, Cook DJ. Crystalloids vs. colloids in fluid resuscitation: A systematic review.Crit Care Med 1999;27:200-10.31. Fehlings MG, Brodke DS, Norvell DC, Dettori JR. The evidence for intraoperative neurophysiological monitoringin spine surgery: Does it make a difference? Spine (Phila Pa 1976) 2010;35:S37-46.32. Erb TO, Ryhult SE, Duitmann E, Hasler C, Luetschg J, Frei FJ. Improvement of motor-evoked potentials byketamine <strong>and</strong> spatial facilitation during spinal surgery in a young child. Anesth Analg 2005;100:1634-6.33. Anschel DJ, Aherne A, Soto RG, Carrion W, Hoegerl C, Nori P, et al. Successful intraoperative spinal cordmonitoring during scoliosis surgery using a total intravenous anesthetic regimen including dexmedetomidine.J Clin Neurophysiol 2008;25:56-61.34. Tobias JD, Goble TJ, Bates G, Anderson JT, Hoernschemeyer DG. Effects of dexmedetomidine on intraoperativemotor <strong>and</strong> somatosensory evoked potential monitoring during spinal surgery in adolescents. Paediatr Anaesth2008;18:1082-8.