12 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Management of opioid side effects – a personal view 13CONSTIPATIONThis is probably the most frequently encountered side effect of opioids, occurring in 72% of cancer patients onmorphine in one study. 15,16 Accurate measurements of incidence of constipation are probably not possible, but frombest estimates, constipation occurs in approximately 10% of the general population, 20% of those over 65 yearsof age, 50% of those with cancer, 70% of patients with advanced cancer, rising to 90% or more in those withadvanced cancer being treated with opioids. Strictly speaking, the term “opioid bowel dysfunction” 17 is perhapsmore accurate <strong>and</strong> often encountered in the literature, but the definition is problematic, <strong>and</strong> varies from publicationto publication. Perhaps the most practical definition for the patient is the experience of less frequent bowel motionsor the sensation that more frequent bowel movements are required.In cancer patients, there are contributing factors to be considered: cancer – related causes, medication related<strong>and</strong> those due to other causes. For example, bed rest, pelvic cancers, bowel obstruction, hypercalcaemia <strong>and</strong>dehydration are not uncommon in a cancer patient population. Some drugs such as chemotherapy agents (eg.vincristine), some antiemetics such as 5HT3 antagonists, antispasmodics, anticholinergics, diuretics <strong>and</strong> ironsupplements can all contribute to constipation. Other conditions such as hypothyrodism, autonomic neuropathy<strong>and</strong> diabetes may also exacerbate constipation from other causes.The pathophysiology of constipation in patients with cancer treated with opioids is not fully understood, butinvolves inhibition of opioid receptors in the myenteric plexus, where the circular smooth muscles are more affectedthan longitudinal muscles 18 . Delayed gastric emptying can occur, <strong>and</strong> reduced peristalsis throughout the gastrointestinaltract is thought to be common. Decreased mucosal secretion has been noted, <strong>and</strong> when this occurs in addition toincreased rectal tone, it is not surprising that opioid bowel dysfunction occurs almost universally. The implicationof an increased rectal tone is that some patients with stomas may only require stool softeners (without bowelstimulants) to relieve their constipation.The principles of management of constipation include exclusion of bowel obstruction, finding <strong>and</strong> treating theunderlying cause if relevant <strong>and</strong> treating the contributing factors. I find something as simple as intravenous fluidsfor 24-48hrs, or encouraging patients to be as active as possible, preferably walking around the ward, can be veryhelpful. If pharmacological treatment is required, then the combination of stool softeners <strong>and</strong> stimulants is a usefulstart (eg. sennosides with docusate). Table 1 lists a suggested starting dose equivalent of laxatives for a given levelof opioid dose. There is no published literature except for Mancini et al 19 who calculated a laxative/opioid ratio formorphine of around 0.15 in a study of 49 patients admitted acutely to a hospice, based on the designation of 100mgdocusate plus 8mg senna as one laxative unit (containing more docusate than one Coloxyl with Senna tablet inAustralia). Using their calculations, one might predict a laxative dose of around 2 tablets twice a day for an opioiddose of 60mg per 24hrs, not dissimilar to Table 1. It is important to note that the dose of laxatives needs to betitrated according to individual response. Like nausea, constipation is best managed using laxatives on a preventativebasis: I usually recommend starting a laxative with, or even before, the first dose of opioid, since most laxativesrequire 4-24hrs to work.In the event of constipation not responding to preventative laxatives in about 2-3 days, Table 2 lists a suggestedescalation plan involving agents delivered per rectum. In general, oral laxatives are preferred before rectaladministration, though sometimes both are required. Oils (paraffin, olive oil) can be administered via the oral routeor as enemas, <strong>and</strong> are also occasionally useful in severe impaction, though manual evacuation is more reliable.Oils are not recommended for chronic use. In patients in whom I am interested in taking an aggressive approachto constipation, overcorrection of constipation may be acceptable before dose reduction of laxatives.In practice, I like to use abdominal X-rays if patients have been constipated for some time, in order to rule outbowel obstruction, though this is not always recommended in the literature. Most radiologists however, do notcomment on constipation or faecal loading, <strong>and</strong> reports generally focus on ruling out acute abdominal events suchas bowel obstruction. As a result, it is always best to visualise the X-rays directly. Also, overflow incontinence isperhaps under-recognised, <strong>and</strong> without a careful history, one can be fooled by the apparent clearing of chronicconstipation.SEDATIONSedation is a common problem, but tends to be mild, occurs early <strong>and</strong> at increases of opioid dose 20 . Tolerancetypically develops in about 2-3 days. For this reason, <strong>and</strong> because continual changes in doses of narcotics areunhelpful, any change in dose of opioids is best done only every 2-3 days, in my view, unless of course it becomesclear that pain is not adequately controlled. In this situation however, sedation is not usually an issue, <strong>and</strong> the mainproblem is inadequate analgesia. Occasionally, sedation fluctuates, in which case strategies could include smalldoses of methylphenidate, possibly modafinil or even a small dose of steroids. If sedation is accompanied byrespiratory depression, then reducing the dose of opioid is the best way to manage the problem. Naloxone can betitrated to effect if used judiciously, but in cancer patients in whom pain control has been an issue, naloxone is bestavoided altogether in view of the potential to cause severe rebound pain.HALLUCINATIONSNon-opioid causes for hallucinations are perhaps more common than narcotics in cancer patients. 20 Cerebralmetastases, particularly if hallucinations in the setting of advanced disease are the first presentation, sepsis, hypoxia,<strong>and</strong> hypercalcaemia are not uncommon causes. Assuming these have been excluded, management includes dosereduction of opioids, small doses of haloperidol (eg. 0.5mg bd), or risperidone (0.5-1.0mg bd). For more prolongedepisodes of hallucinations or delirium, palliative care physicians sometimes prescribe higher doses of haloperidol,risperidone, olanzapine or chlorpromazine.DRY MOUTHThis is a common, though generally mild, side effect associated with opioids. Symptomatic treatment is all that isusually required if it is a feature in the patient’s complaints.OTHER SIDE EFFECTSItch is occasionally an issue, <strong>and</strong> has been estimated to occur in around 1% of patients treated with opioids, risingto 40% with the use of spinal opioids, suggesting a spinal opioid receptor mechanism. 21 The cause is unclear, <strong>and</strong>may be dose related. There is some evidence that opioids cause some histamine release from mast cells (thoughthis has not been demonstrated for fentanyl <strong>and</strong> sufentanil, though curiously, itching still can occur with the use ofthese drugs). Treatment is again symptomatic, with a trial of antihistamines worthwhile. Physical treatments suchas cool compresses <strong>and</strong> moisturisers may be helpful.Myoclonus may be more frequent with chronic use, <strong>and</strong> the risk appears to increase in the presence of spinalcord lesions in patients. 22 It may also be related to reduced clearance of opioid metabolites, though there is nogood evidence in this regard. In the presence of persistent myoclonus, opioid rotation (morphine, hydromorphone,oxycodone, fentanyl, methadone) has been suggested. 22 If this approach fails, gabapentin 23 lorazepam or clonazepammay be useful.NEW DRUGS AND APPROACHESIn the last decade, a number of novel drugs have been developed that target the most common side effect ofopioids: constipation. Recent meta-analyses 24,25 suggest that both methylnaltrexone <strong>and</strong> alvimopam have Level 1evidence to show that they are better than placebo in treating constipation <strong>and</strong> post-operative ileus.Methylnaltrexone is a peripheral mu-opioid receptor antagonist that does not cross the blood brain barrier inappreciable amounts <strong>and</strong> as a result, does not antagonise opioid induced central nervous system effects such assedation. 26,27 In Australia, it is approved on the pharmaceutical benefits scheme. A subcutaneous dose results in abowel movement around 4 hours later, but occasionally a second dose may be required. Given its apparent abilityto “rescue” patients with constipation, it is generally not used as first line treatment, <strong>and</strong> tends to be reserved forpatients who fail st<strong>and</strong>ard laxatives.Alvimopam is also a peripheral mu-opioid receptor antagonist that does not cross the blood brain barrier inappreciable amounts. 27 It was approved by the American Federal Drug Agency (FDA) in 2008 for use for postoperativeileus. 28 For this indication, it is commenced prior to surgery <strong>and</strong> administered twice a day for a week. Thedrug is well-tolerated.Phase III trials of an oxycodone/naloxone combination show that significantly less constipation occurs with itsuse than oxycodone. 29,30 The rationale behind this is the pharmacological advantage of giving naloxone orally, whichhas low bioavailability <strong>and</strong> which exclusively inhibits gut opioid receptors. However, side effects from the oxycodonecomponent can occur, not unexpectedly.Tapentadol is a mu-opioid receptor activator <strong>and</strong> noradrenaline reuptake blocker that acts in the central nervoussystem. 31 It is useful in a variety of pain conditions, including back pain <strong>and</strong> osteoarthritis. 32 It has already beenFDA approved <strong>and</strong> appears to cause less constipation than oxycodone in clinical trials.PHARMACOGENETICSAlthough in its infancy, the study of pharmacogenetics of opioids appears to be taking shape. It may be possibletherefore, to identify patients who have a higher risk of severe or unusual reactions to opioids prior to the developmentof these adverse events. 33 For instance, genetic polymorphisms of cytochrome P4502D6 may help to determinerapid metabolisers of codeine (into morphine, more side effects) from those who are poor metabolisers (more pain),(see Kadiev et al, 2008 for review). 34CONCLUSIONSAlthough opioids are extremely useful in the management of pain syndromes in many different diseases, patientscommonly experience side effects. Fortunately, most of these are either mild or manageable. The incidence of theseadverse events can only be estimated from large clinical trials, but these patient populations are unlikely to representthe “real world” where patients have generally poorer performance status, or may have multiple co-morbiditieswhich increase the risk of side effects. If we assume recent pharmacogenetic work is a reasonable guide, thenapproximately 10% of patients have unusual or more severe side effects than most patients, while 10% of patientscould be expected to have poor pain control with st<strong>and</strong>ard opioid <strong>and</strong> adjunct treatment approaches. It wouldseem that these patients may benefit most from the novel drugs recently developed, which of course would alsobe suitable for patients in whom side effects of opioids such as constipation are difficult to manage.
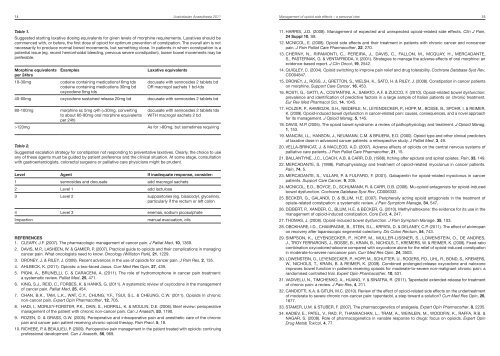
14 <strong>Australasian</strong> <strong>Anaesthesia</strong> <strong>2011</strong>Management of opioid side effects – a personal view 15Table 1.Suggested starting laxative dosing equivalents for given levels of morphine requirements. Laxatives should becommenced with, or before, the first dose of opioid for optimum prevention of constipation. The overall aim is notnecessarily to produce normal bowel movements, but something close. In patients in whom constipation is apotential issue (eg. recent hemorrhoidal bleeding, previous severe constipation), looser bowel movements may bepreferable.Morphine equivalentsper 24hrs10-30mgExamplescodeine containing medications16mg tdscodeine containing medications 30mg bdoxycodone 5mg tdsLaxative equivalentsdocusate with sennosides 2 tablets bdOR macrogol sachets 1 bd-tds40-60mg oxycodone sustained release 20mg bd docusate with sennosides 2 tablets bd80-100mg>120mgmorphine sc 5mg q4h (=30mg, convertingto about 60-90mg oral morphine equivalentsper 24h)docusate with sennosides 2 tablets tdsWITH macrogol sachets 2 bdAs for >80mg, but sometimes requiringTable 2.Suggested escalation strategy for constipation not responding to preventative laxatives. Clearly, the choice to useany of these agents must be guided by patient preference <strong>and</strong> the clinical situation. At some stage, consultationwith gastroenterologists, colorectal surgeons or palliative care physicians might be prudent.Level Agent If inadequate response, consider:1 sennosides <strong>and</strong> docusate add macrogol sachets2 Level 1 add lactulose3 Level 2 suppositories (eg. bisacodyl, glycerine),particularly if the rectum or left colon4 Level 3 enemas, sodium picosulphateImpactionmanual evacuation, oilsREFERENCES1. CLEARY, J.F. (2007). The pharmacologic management of cancer pain. J Palliat Med, 10, 1369.2. DAVIS, M.P., LASHEEN, W. & GAMIER, P. (2007). Practical guide to opioids <strong>and</strong> their complications in managingcancer pain. What oncologists need to know. Oncology (Williston Park), 21, 1229.3. DRONEY, J. & RILEY, J. (2009). Recent advances in the use of opioids for cancer pain. J Pain Res, 2, 135.4. AHLBECK, K. (<strong>2011</strong>). Opioids: a two-faced Janus. Curr Med Res Opin, 27, 439.5. PIGNI, A., BRUNELLI, C. & CARACENI, A. (<strong>2011</strong>). The role of hydromorphone in cancer pain treatment:a systematic review. Palliat Med, 25, 471.6. KING, S.J., REID, C., FORBES, K. & HANKS, G. (<strong>2011</strong>). A systematic review of oxycodone in the managementof cancer pain. Palliat Med, 25, 454.7. CHAN, B.K., TAM, L.K., WAT, C.Y., CHUNG, Y.F., TSUI, S.L. & CHEUNG, C.W. (<strong>2011</strong>). Opioids in chronicnon-cancer pain. Expert Opin Pharmacother, 12, 705.8. HADI, I., MORLEY-FORSTER, P.K., DAIN, S., HORRILL, K. & MOULIN, D.E. (2006). Brief review: perioperativemanagement of the patient with chronic non-cancer pain. Can J Anaesth, 53, 1190.9. ROZEN, D. & GRASS, G.W. (2005). Perioperative <strong>and</strong> intraoperative pain <strong>and</strong> anesthetic care of the chronicpain <strong>and</strong> cancer pain patient receiving chronic opioid therapy. Pain Pract, 5, 18.10. RICHEBE, P. & BEAULIEU, P. (2009). Perioperative pain management in the patient treated with opioids: continuingprofessional development. Can J Anaesth, 56, 969.11. HARRIS, J.D. (2008). Management of expected <strong>and</strong> unexpected opioid-related side effects. Clin J Pain,24 Suppl 10, S8.12. MCNICOL, E. (2008). Opioid side effects <strong>and</strong> their treatment in patients with chronic cancer <strong>and</strong> noncancerpain. J Pain Palliat Care Pharmacother, 22, 270.13. CHERNY, N., RIPAMONTI, C., PEREIRA, J., DAVIS, C., FALLON, M., MCQUAY, H., MERCADANTE,S., PASTERNAK, G. & VENTAFRIDDA, V. (2001). Strategies to manage the adverse effects of oral morphine: anevidence-based report. J Clin Oncol, 19, 2542.14. QUIGLEY, C. (2004). Opioid switching to improve pain relief <strong>and</strong> drug tolerability. Cochrane Database Syst Rev,CD004847.15. DRONEY, J., ROSS, J., GRETTON, S., WELSH, K., SATO, H. & RILEY, J. (2008). Constipation in cancer patientson morphine. Support Care Cancer, 16, 453.16. ROSTI, G., GATTI, A., COSTANTINI, A., SABATO, A.F. & ZUCCO, F. (2010). Opioid-related bowel dysfunction:prevalence <strong>and</strong> identification of predictive factors in a large sample of Italian patients on chronic treatment.Eur Rev Med Pharmacol Sci, 14, 1045.17. HOLZER, P., AHMEDZAI, S.H., NIEDERLE, N., LEYENDECKER, P., HOPP, M., BOSSE, B., SPOHR, I. & REIMER,K. (2009). Opioid-induced bowel dysfunction in cancer-related pain: causes, consequences, <strong>and</strong> a novel approachfor its management. J Opioid Manag, 5, 145.18. DAVIS, M.P. (2005). The opioid bowel syndrome: a review of pathophysiology <strong>and</strong> treatment. J Opioid Manag,1, 153.19. MANCINI, I.L., HANSON, J., NEUMANN, C.M. & BRUERA, E.D. (2000). Opioid type <strong>and</strong> other clinical predictorsof laxative dose in advanced cancer patients: a retrospective study. J Palliat Med, 3, 49.20. VELLA-BRINCAT, J. & MACLEOD, A.D. (2007). Adverse effects of opioids on the central nervous systems ofpalliative care patients. J Pain Palliat Care Pharmacother, 21, 15.21. BALLANTYNE, J.C., LOACH, A.B. & CARR, D.B. (1988). Itching after epidural <strong>and</strong> spinal opiates. Pain, 33, 149.22. MERCADANTE, S. (1998). Pathophysiology <strong>and</strong> treatment of opioid-related myoclonus in cancer patients.Pain, 74, 5.23. MERCADANTE, S., VILLARI, P. & FULFARO, F. (2001). Gabapentin for opioid-related myoclonus in cancerpatients. Support Care Cancer, 9, 205.24. MCNICOL, E.D., BOYCE, D., SCHUMANN, R. & CARR, D.B. (2008). Mu-opioid antagonists for opioid-inducedbowel dysfunction. Cochrane Database Syst Rev, CD006332.25. BECKER, G., GALANDI, D. & BLUM, H.E. (2007). Peripherally acting opioid antagonists in the treatment ofopiate-related constipation: a systematic review. J Pain Symptom Manage, 34, 547.26. DEIBERT, P., XANDER, C., BLUM, H.E. & BECKER, G. (2010). Methylnaltrexone: the evidence for its use in themanagement of opioid-induced constipation. Core Evid, 4, 247.27. THOMAS, J. (2008). Opioid-induced bowel dysfunction. J Pain Symptom Manage, 35, 103.28. OBOKHARE, I.D., CHAMPAGNE, B., STEIN, S.L., KRPATA, D. & DELANEY, C.P. (<strong>2011</strong>). The effect of alvimopanon recovery after laparoscopic segmental colectomy. Dis Colon Rectum, 54, 743.29. SIMPSON, K., LEYENDECKER, P., HOPP, M., MULLER-LISSNER, S., LOWENSTEIN, O., DE ANDRES,J., TROY FERRARONS, J., BOSSE, B., KRAIN, B., NICHOLS, T., KREMERS, W. & REIMER, K. (2008). Fixed-ratiocombination oxycodone/naloxone compared with oxycodone alone for the relief of opioid-induced constipationin moderate-to-severe noncancer pain. Curr Med Res Opin, 24, 3503.30. LOWENSTEIN, O., LEYENDECKER, P., HOPP, M., SCHUTTER, U., ROGERS, P.D., UHL, R., BOND, S., KREMERS,W., NICHOLS, T., KRAIN, B. & REIMER, K. (2009). Combined prolonged-release oxycodone <strong>and</strong> naloxoneimproves bowel function in patients receiving opioids for moderate-to-severe non-malignant chronic pain: ar<strong>and</strong>omised controlled trial. Expert Opin Pharmacother, 10, 531.31. VADIVELU, N., TIMCHENKO, A., HUANG, Y. & SINATRA, R. (<strong>2011</strong>). Tapentadol extended-release for treatmentof chronic pain: a review. J Pain Res, 4, 211.32. CANDIOTTI, K.A. & GITLIN, M.C. (2010). Review of the effect of opioid-related side effects on the undertreatmentof moderate to severe chronic non-cancer pain: tapentadol, a step toward a solution? Curr Med Res Opin, 26,1677.33. STAMER, U.M. & STUBER, F. (2007). The pharmacogenetics of analgesia. Expert Opin Pharmacother, 8, 2235.34. KADIEV, E., PATEL, V., RAD, P., THANKACHAN, L., TRAM, A., WEINLEIN, M., WOODFIN, K., RAFFA, R.B. &NAGAR, S. (2008). Role of pharmacogenetics in variable response to drugs: focus on opioids. Expert OpinDrug Metab Toxicol, 4, 77.