Fortbildungen / Formations continues 2012 - IUMSP
Fortbildungen / Formations continues 2012 - IUMSP
Fortbildungen / Formations continues 2012 - IUMSP

Erfolgreiche ePaper selbst erstellen
Machen Sie aus Ihren PDF Publikationen ein blätterbares Flipbook mit unserer einzigartigen Google optimierten e-Paper Software.
DER SELTENE FALL<br />
CASTLE «Carcinoma<br />
showing thymus-like<br />
differentiation of the<br />
thyroid»: a rare cause<br />
of neck mass<br />
M. Zare, S. Cochet, M. Pusztaszeri, P. -Y. Dietrich<br />
Keywords: CASTLE, solid cell nests, CD5<br />
Introduction<br />
The presence of a mass in the neck gives rise to a wide<br />
differential diagnosis, ranging from benign to serious aetiologies.<br />
Congenital neck masses are usually present at<br />
birth and are often cysts originating from branchial clefts<br />
or the thyroglossal duct. In�ammatory neck masses are<br />
generally related to enlarged lymph nodes and have various<br />
infectious origins. Malignant diseases have always to<br />
be considered in case of neck masses. The most common<br />
cancers are metastatic lymph nodes from head and neck<br />
squamous cell carcinomas, thyroid tumours or lymphomas.<br />
Rare (e.g., paraganglioma or schwannoma) or even<br />
exceptional tumours should also be included in the differential<br />
diagnosis, such as CASTLE tumour.<br />
Case report<br />
A 58–year-old Caucasian man developed hoarseness and occasional<br />
dysphagia to liquids and solids in 2010. Clinical<br />
examination revealed a palsy of the left vocal cord and a<br />
slightly painful left neck mass. The total body scan showed<br />
a 4 cm sized left neck mass attached to the inferior part of<br />
the thyroid (Figure 1). A �ne needle aspiration biopsy was<br />
not conclusive. Panendoscopy was normal. Neck MRI con-<br />
�rmed the presence of a mass with apparent involvement of<br />
both the thyroid and the trachea, and suspicious left para-<br />
and pre-tracheal nodes. A surgical biopsy was performed<br />
and the diagnosis of moderately to poorly differentiated<br />
squamous cell carcinoma was established. The patient underwent<br />
total removal of the mass with tumorectomy, dissection<br />
of group IV lymph nodes, left hemi-thyroidectomy<br />
and resection of the third to the �fth tracheal rings.<br />
The resection specimen showed a whitish and �brotic mass<br />
partly invading the thyroid, and extending to the tracheal<br />
rings and the skeletal muscles with macroscopically positive<br />
surgical margins. Microscopically, �brous septa surrounded<br />
large irregular nests of poorly differentiated ovoid<br />
cells with an amphophilic cytoplasm, round nucleus,<br />
�ne granular chromatin and central nucleoli (Figure 2).<br />
There were a few number of mitosis and rare images of pe-<br />
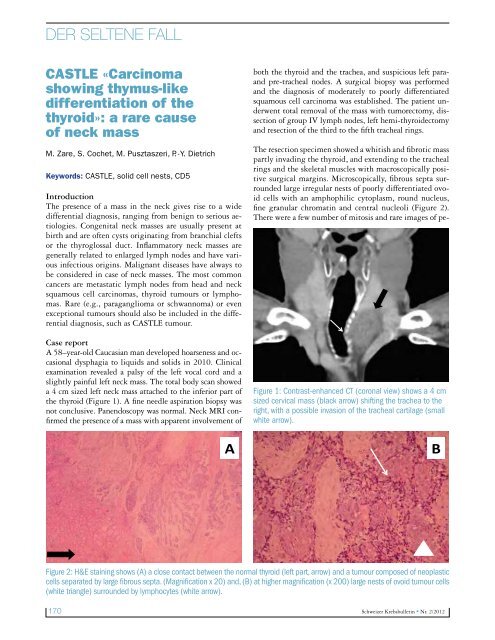
Figure 1: Contrast-enhanced CT (coronal view) shows a 4 cm<br />
sized cervical mass (black arrow) shifting the trachea to the<br />
right, with a possible invasion of the tracheal cartilage (small<br />
white arrow).<br />
A B<br />
Figure 2: H&E staining shows (A) a close contact between the normal thyroid (left part, arrow) and a tumour composed of neoplastic<br />
cells separated by large �brous septa. (Magni�cation x 20) and, (B) at higher magni�cation (x 200) large nests of ovoid tumour cells<br />
(white triangle) surrounded by lymphocytes (white arrow).<br />
170 Schweizer Krebsbulletin � Nr. 2/<strong>2012</strong>