

Afghanistan Mortality Survey 2010 - Measure DHS
Afghanistan Mortality Survey 2010 - Measure DHS
Afghanistan Mortality Survey 2010 - Measure DHS
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
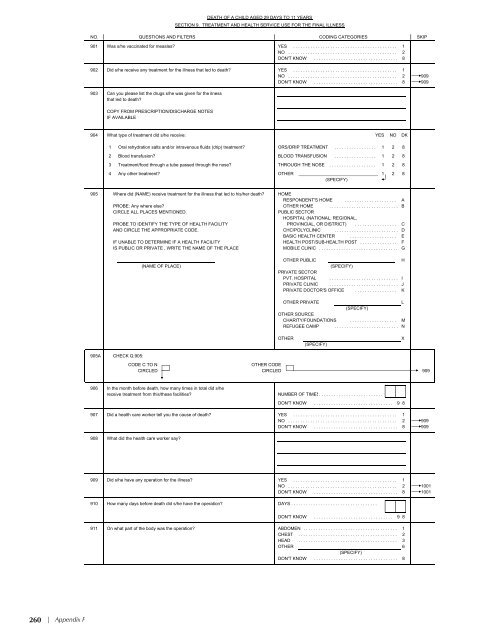
NO. QUESTIONS AND FILTERS CODING CATEGORIES SKIP901 Was s/he vaccinated for measles? YES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1NO . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8902 Did s/he receive any treatment for the illness that led to death? YES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1NO . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 909DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 909903 Can you please list the drugs s/he was given for the ilnessthat led to death?COPY FROM PRESCRIPTION/DISCHARGE NOTESIF AVAILABLEDEATH OF A CHILD AGED 29 DAYS TO 11 YEARSSECTION 9. TREATMENT AND HEALTH SERVICE USE FOR THE FINAL ILLNESS904 What type of treatment did s/he receive: YES NO DK1 Oral rehydration salts and/or intravenous fluids (drip) treatment? ORS/DRIP TREATMENT . . . . . . . . . . . . . . . . . 1 2 82 Blood transfusion? BLOOD TRANSFUSION . . . . . . . . . . . . . . . . . 1 2 83 Treatment/food through a tube passed through the nose? THROUGH THE NOSE . . . . . . . . . . . . . . . . . . . 1 2 84 Any other treatment? OTHER ________________________________ 1 2 8(SPECIFY)905 Where did (NAME) receive treatment for the illness that led to his/her death? HOMERESPONDENT'S HOME . . . . . . . . . . . . . . . . . . . . . APROBE: Any where else? OTHER HOME . . . . . . . . . . . . . . . . . . . . . . . . . . . . BCIRCLE ALL PLACES MENTIONED.PUBLIC SECTORHOSPITAL (NATIONAL, REGIONAL,PROBE TO IDENTIFY THE TYPE OF HEALTH FACILITY PROVINCIAL, OR DISTRICT) . . . . . . . . . . . . . . . . . CAND CIRCLE THE APPROPRIATE CODE. CHC/POLYCLINIC . . . . . . . . . . . . . . . . . . . . . . . . . . DBASIC HEALTH CENTER . . . . . . . . . . . . . . . . . . . EIF UNABLE TO DETERMINE IF A HEALTH FACILITY HEALTH POST/SUB-HEALTH POST . . . . . . . . . . . . . . . FIS PUBLIC OR PRIVATE , WRITE THE NAME OF THE PLACEMOBILE CLINIC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . G(NAME OF PLACE)OTHER PUBLICH(SPECIFY)PRIVATE SECTORPVT. HOSPITAL . . . . . . . . . . . . . . . . . . . . . . . . . . . . IPRIVATE CLINIC . . . . . . . . . . . . . . . . . . . . . . . . . . . . JPRIVATE DOCTOR'S OFFICE . . . . . . . . . . . . . . . . . KOTHER PRIVATEL(SPECIFY)OTHER SOURCECHARITY/FOUNDATIONS . . . . . . . . . . . . . . . . . . . MREFUGEE CAMP . . . . . . . . . . . . . . . . . . . . . . . . . . NOTHER(SPECIFY)X905ACHECK Q.905:CODE C TO NOTHER CODECIRCLED CIRCLED 909906 In the month before death, how many times in total did s/hereceive treatment from this/these facilities? NUMBER OF TIMES. . . . . . . . . . . . . . . . . . . . . . . . . .DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 8907 Did a health care worker tell you the cause of death? YES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1NO . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 909DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 909908 What did the health care worker say?909 Did s/he have any operation for the illness? YES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1NO . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 1001DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8 1001910 How many days before death did s/he have the operation? DAYS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 8911 On what part of the body was the operation? ABDOMEN . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1CHEST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2HEAD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3OTHER 6(SPECIFY)DON'T KNOW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8260 | Appendix F





![Obtaining Informed Consent for HIV Testing [QRS4] - Measure DHS](https://img.yumpu.com/49850117/1/190x245/obtaining-informed-consent-for-hiv-testing-qrs4-measure-dhs.jpg?quality=85)








