Bariatric treatments for adult obesity - Institute of Health Economics
Bariatric treatments for adult obesity - Institute of Health Economics
Bariatric treatments for adult obesity - Institute of Health Economics
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
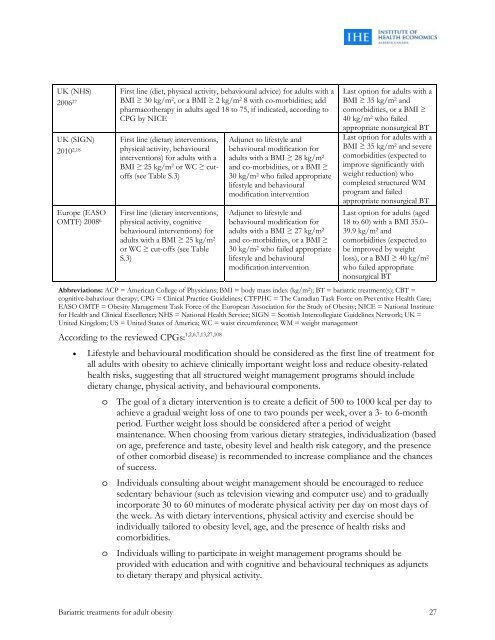
UK (NHS)2006 27UK (SIGN)2010 2,18Europe (EASOOMTF) 2008 6First line (diet, physical activity, behavioural advice) <strong>for</strong> <strong>adult</strong>s with aBMI ≥ 30 kg/m 2 , or a BMI ≥ 2 kg/m 2 8 with co-morbidities; addpharmacotherapy in <strong>adult</strong>s aged 18 to 75, if indicated, according toCPG by NICEFirst line (dietary interventions,physical activity, behaviouralinterventions) <strong>for</strong> <strong>adult</strong>s with aBMI ≥ 25 kg/m 2 or WC ≥ cut<strong>of</strong>fs(see Table S.3)First line (dietary interventions,physical activity, cognitivebehavioural interventions) <strong>for</strong><strong>adult</strong>s with a BMI ≥ 25 kg/m 2or WC ≥ cut-<strong>of</strong>fs (see TableS.3)Adjunct to lifestyle andbehavioural modification <strong>for</strong><strong>adult</strong>s with a BMI ≥ 28 kg/m 2and co-morbidities, or a BMI ≥30 kg/m 2 who failed appropriatelifestyle and behaviouralmodification interventionAdjunct to lifestyle andbehavioural modification <strong>for</strong><strong>adult</strong>s with a BMI ≥ 27 kg/m 2and co-morbidities, or a BMI ≥30 kg/m 2 who failed appropriatelifestyle and behaviouralmodification interventionLast option <strong>for</strong> <strong>adult</strong>s with aBMI ≥ 35 kg/m 2 andcomorbidities, or a BMI ≥40 kg/m 2 who failedappropriate nonsurgical BTLast option <strong>for</strong> <strong>adult</strong>s with aBMI ≥ 35 kg/m 2 and severecomorbidities (expected toimprove significantly withweight reduction) whocompleted structured WMprogram and failedappropriate nonsurgical BTLast option <strong>for</strong> <strong>adult</strong>s (aged18 to 60) with a BMI 35.0–39.9 kg/m 2 andcomorbidities (expected tobe improved by weightloss), or a BMI ≥ 40 kg/m 2who failed appropriatenonsurgical BTAbbreviations: ACP = American College <strong>of</strong> Physicians; BMI = body mass index (kg/m 2 ); BT = bariatric treatment(s); CBT =cognitive-bahaviour therapy; CPG = Clinical Practice Guidelines; CTFPHC = The Canadian Task Force on Preventive <strong>Health</strong> Care;EASO OMTF = Obesity Management Task Force <strong>of</strong> the European Association <strong>for</strong> the Study <strong>of</strong> Obesity; NICE = National <strong>Institute</strong><strong>for</strong> <strong>Health</strong> and Clinical Excellence; NHS = National <strong>Health</strong> Service; SIGN = Scottish Intercollegiate Guidelines Network; UK =United Kingdom; US = United States <strong>of</strong> America; WC = waist circumference; WM = weight managementAccording to the reviewed CPGs: 1,2,6,7,13,27,108Lifestyle and behavioural modification should be considered as the first line <strong>of</strong> treatment <strong>for</strong>all <strong>adult</strong>s with <strong>obesity</strong> to achieve clinically important weight loss and reduce <strong>obesity</strong>-relatedhealth risks, suggesting that all structured weight management programs should includedietary change, physical activity, and behavioural components.o The goal <strong>of</strong> a dietary intervention is to create a deficit <strong>of</strong> 500 to 1000 kcal per day toachieve a gradual weight loss <strong>of</strong> one to two pounds per week, over a 3- to 6-monthperiod. Further weight loss should be considered after a period <strong>of</strong> weightmaintenance. When choosing from various dietary strategies, individualization (basedon age, preference and taste, <strong>obesity</strong> level and health risk category, and the presence<strong>of</strong> other comorbid disease) is recommended to increase compliance and the chances<strong>of</strong> success.o Individuals consulting about weight management should be encouraged to reducesedentary behaviour (such as television viewing and computer use) and to graduallyincorporate 30 to 60 minutes <strong>of</strong> moderate physical activity per day on most days <strong>of</strong>the week. As with dietary interventions, physical activity and exercise should beindividually tailored to <strong>obesity</strong> level, age, and the presence <strong>of</strong> health risks andcomorbidities.o Individuals willing to participate in weight management programs should beprovided with education and with cognitive and behavioural techniques as adjunctsto dietary therapy and physical activity.<strong>Bariatric</strong> <strong>treatments</strong> <strong>for</strong> <strong>adult</strong> <strong>obesity</strong> 27