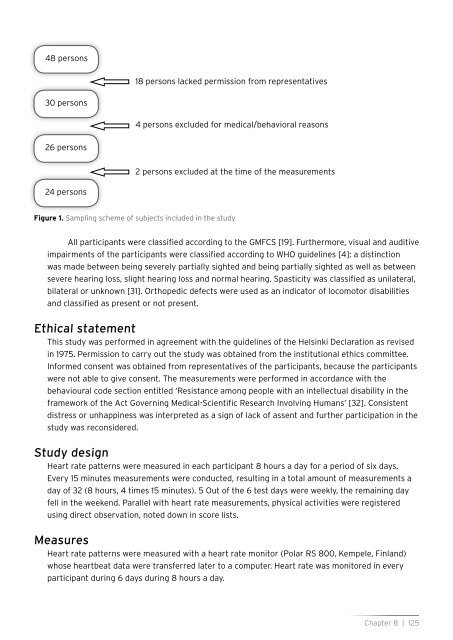
48 persons18 persons lacked permission from representatives30 persons4 persons excluded for medical/behavioral reasons26 persons2 persons excluded at the time of the measurements24 personsFigure 1. Sampl<strong>in</strong>g scheme of subjects <strong>in</strong>cluded <strong>in</strong> the studyAll participants were classified accord<strong>in</strong>g to the GMFCS [19]. Furthermore, visual and auditiveimpairments of the participants were classified accord<strong>in</strong>g to WHO guidel<strong>in</strong>es [4]: a dist<strong>in</strong>ctionwas made between be<strong>in</strong>g severely partially sighted and be<strong>in</strong>g partially sighted as well as betweensevere hear<strong>in</strong>g loss, slight hear<strong>in</strong>g loss and normal hear<strong>in</strong>g. Spasticity was classified as unilateral,bilateral or unknown [31]. Orthopedic defects were used as an <strong>in</strong>dicator of locomotor disabilitiesand classified as present or not present.Ethical statementThis study was performed <strong>in</strong> agreement <strong>with</strong> the guidel<strong>in</strong>es of the Hels<strong>in</strong>ki Declaration as revised<strong>in</strong> 1975. Permission to carry out the study was obta<strong>in</strong>ed from the <strong>in</strong>stitutional ethics committee.Informed consent was obta<strong>in</strong>ed from representatives of the participants, because the participantswere not able to give consent. The measurements were performed <strong>in</strong> accordance <strong>with</strong> thebehavioural code section entitled ‘Resistance among people <strong>with</strong> an <strong>in</strong>tellectual disability <strong>in</strong> theframework of the Act Govern<strong>in</strong>g Medical-Scientific Research Involv<strong>in</strong>g Humans’ [32]. Consistentdistress or unhapp<strong>in</strong>ess was <strong>in</strong>terpreted as a sign of lack of assent and further participation <strong>in</strong> thestudy was reconsidered.Study designHeart rate patterns were measured <strong>in</strong> each participant 8 hours a day for a period of six days.Every 15 m<strong>in</strong>utes measurements were conducted, result<strong>in</strong>g <strong>in</strong> a total amount of measurements aday of 32 (8 hours, 4 times 15 m<strong>in</strong>utes). 5 Out of the 6 test days were weekly, the rema<strong>in</strong><strong>in</strong>g dayfell <strong>in</strong> the weekend. Parallel <strong>with</strong> heart rate measurements, <strong>physical</strong> activities were registeredus<strong>in</strong>g direct observation, noted down <strong>in</strong> score lists.MeasuresHeart rate patterns were measured <strong>with</strong> a heart rate monitor (Polar RS 800, Kempele, F<strong>in</strong>land)whose heartbeat data were transferred later to a computer. Heart rate was monitored <strong>in</strong> everyparticipant dur<strong>in</strong>g 6 days dur<strong>in</strong>g 8 hours a day.Chapter 8 | 125
Data regard<strong>in</strong>g <strong>physical</strong> activity were registered <strong>with</strong> the use of a questionnaire, which wasfilled out by both personal caregivers at the liv<strong>in</strong>g group as support staff of the activity centre.Physical activity was coded as ‘Targeted <strong>physical</strong> activity Yes’ or ‘Targeted <strong>physical</strong> activity No’.Mov<strong>in</strong>g <strong>with</strong> the wheelchair <strong>in</strong>side or outside, transfer, active sitt<strong>in</strong>g <strong>with</strong>out support, gymnastics<strong>with</strong> a gymnastic <strong>in</strong>structor, <strong>physical</strong> therapy, play<strong>in</strong>g <strong>with</strong> a ball, and ‘danc<strong>in</strong>g’ on music were allexamples of ‘Targeted <strong>physical</strong> activity Yes’. Listen<strong>in</strong>g to music, watch<strong>in</strong>g television or ly<strong>in</strong>g downon a bed were all examples of “Targeted <strong>physical</strong> activity No’.Data analysisHeart rate zonesPeak heart rate, rest heart rate and heart rate reserves differ for each person, which makes themdifficult to compare. By calculat<strong>in</strong>g heart rate zones accord<strong>in</strong>g to the equation of Karvonen [33], itis possible to compare the zones of the participants <strong>with</strong> each other.Heart rate zones are calculated as follows. First, each participant’s peak heart rate wasestimated us<strong>in</strong>g the formula of Fernhall [34] for participants <strong>with</strong> <strong>in</strong>tellectual disabilities: 210 –0.56 (age) – 15.5. Due to the motor disabilities of the participants, no other non-<strong>in</strong>vasive measurecould be performed. Secondly, the participants rest<strong>in</strong>g heart rate was determ<strong>in</strong>ed by tak<strong>in</strong>g themedian of fifteen morn<strong>in</strong>g heart rate measurements. Thirdly, us<strong>in</strong>g the participants rest<strong>in</strong>g heartrate, the heart rate reserve was calculated by subtract<strong>in</strong>g rest<strong>in</strong>g heart rate of estimated peakheart rate. F<strong>in</strong>ally, the heart rate reserve was divided <strong>in</strong> 10 zones, each zone consist<strong>in</strong>g of 10%of the heart rate reserve. The heart rate of a participant dur<strong>in</strong>g each 15 m<strong>in</strong>utes was classified <strong>in</strong>these zones. For <strong>in</strong>stance: rest<strong>in</strong>g heart rate of 50 beats per m<strong>in</strong>ute (bpm), maximum heart rate of180 bpm; heart rate reserve is 130 bpm; each heart rate zone exists of 13 heart rates, the first zoneis from 50 to 63; the second from 63 to 76; and so on (Table 1).Table 1. Example of the heart rate zones for healthy personsHeart Rate Zone Activity Percentage of heart rate reserve (HRV)1 50-63 Rest 1-102 63-77 10-203 77-90 Quiet mov<strong>in</strong>g 20-304 90-103 30-405 103-116 Moderately <strong>in</strong>tensive activity 40-506 116-129 ACSM guidel<strong>in</strong>e of healthy <strong>physical</strong> activity 50-607 129-142 Intensive activity 60-708 142-155 70-809 155-168 Very <strong>in</strong>tensive activity 80-9010 168-180 90-100Patterns and classes <strong>in</strong> heart rateHeart rate of the 24 participants was measured eight hours a day dur<strong>in</strong>g six days, <strong>with</strong>measurements be<strong>in</strong>g conducted every 15 m<strong>in</strong>utes. In order to determ<strong>in</strong>e the activity levels ofpersons <strong>with</strong> PIMD compared <strong>with</strong> ACSM guidel<strong>in</strong>es of healthy <strong>physical</strong> activity, an overview ofthe heart rate zones is presented, along <strong>with</strong> a day to day outl<strong>in</strong>e of the mean prevalence of heartrate zones of the participants.126 | Chapter 8
- Page 2 and 3:
Measuring physical fitnessin person
- Page 4:
Rijksuniversiteit GroningenMeasurin
- Page 10 and 11:
Chapter 1IntroductionChapter 1 | 9
- Page 12 and 13:
overweight [15]. This prevalence is
- Page 14 and 15:
Theoretical framework of the studyI
- Page 16 and 17:
Components of physical fitnessThe a
- Page 18 and 19:
Therefore, a study is put forward w
- Page 20 and 21:
2002;40:436-444.19 Temple VA, Frey
- Page 22 and 23:
Chapter 2Feasibility and reliabilit
- Page 24 and 25:
IntroductionPhysical fitness and he
- Page 26 and 27:
GMFCS was presented to the investig
- Page 28 and 29:
Body weightTo determine the body we
- Page 30 and 31:
Table 1 Results of Wilcoxon rank te
- Page 32 and 33:
Calculation of heightThe mean (SD)
- Page 34 and 35:
DiscussionThe results of our study
- Page 36 and 37:
References1 Bouchard C, Shepard RJ,
- Page 38 and 39:
37 Rimmer J, Kelly LE, Rosentswieg
- Page 40 and 41:
Chapter 3Measuring waist circumfere
- Page 42 and 43:
IntroductionChildren and adults wit
- Page 44 and 45:
participants. These calculations as
- Page 46 and 47:
Data analysisThe data were analyzed
- Page 48:
Table 2. Simple regression analysis
- Page 54 and 55:
Chapter 4Feasibility and reliabilit
- Page 56 and 57:
IntroductionPeople with intellectua
- Page 58 and 59:
Eighty representatives gave permiss
- Page 60 and 61:
3) The measurement procedure: The m
- Page 62 and 63:
and whether motivation influenced t
- Page 64 and 65:
Table 3. Mean peak heart rate achie
- Page 66 and 67:
AcknowledgementsThis research was f
- Page 68 and 69:
21 Hopkins WG, Gaeta H, Thomas AC,
- Page 70 and 71:
Chapter 5Psychometric quality of a
- Page 72 and 73:
IntroductionIntellectual disability
- Page 74 and 75:
Exclusion criteria were mental or p
- Page 76 and 77: participant had fulfilled the task.
- Page 78 and 79: Table 2. Descriptive results peak h
- Page 80 and 81: Table 3. Test-retest reliability of
- Page 82 and 83: Table 4. Correlation scored motivat
- Page 84 and 85: preceding GXT results on HR peak. G
- Page 86 and 87: References1 Schalock R, Brown I, Br
- Page 88 and 89: 37 Stanish HI, Temple VA, Frey GC.
- Page 90 and 91: Chapter 6Feasibility and reliabilit
- Page 92 and 93: IntroductionLocomotor skills in peo
- Page 94 and 95: this study was to evaluate the feas
- Page 96 and 97: obtained from the legal representat
- Page 98 and 99: Modified Berg Balance Scale scoresI
- Page 100 and 101: Modified Berg Balance Scale scoresT
- Page 102 and 103: References1 Van Erkelens-Zwets JHJ
- Page 104 and 105: 39 Dorai-Raj S. Binomial Confidence
- Page 106 and 107: Chapter 7Feasibility, test-retest r
- Page 108 and 109: IntroductionPersons with profound i
- Page 110 and 111: DesignThe muscle tone and spasticit
- Page 112 and 113: Interrater reliabilityFirstly, to d
- Page 114 and 115: Table 3. Summary of the statistical
- Page 116 and 117: Table 6. Summary of the statistical
- Page 118 and 119: RecommendationsThe feasibility of c
- Page 120 and 121: 18 Gielen EJJM. Is spasticiteit te
- Page 122 and 123: Chapter 8Heart Rate Pattern as an I
- Page 124 and 125: IntroductionIt is important to gain
- Page 128 and 129: Furthermore, the mean and the range
- Page 130 and 131: Table 3. Day-to-day outline of the
- Page 132 and 133: Relation between heart rate pattern
- Page 134 and 135: patterns in this study we can concl
- Page 136 and 137: References1 Emerson E. Underweight,
- Page 138 and 139: 38 Multilevel Models Project (2004)
- Page 140 and 141: Chapter 9General DiscussionChapter
- Page 142 and 143: on this. To sum up, testing in pers
- Page 144 and 145: for future research it is recommend
- Page 146 and 147: studies. Randomized Controlled Tria
- Page 148 and 149: of these individuals require more?
- Page 150 and 151: 19 Lahtinen U, Rintala P, Malin A.
- Page 152 and 153: SummarySummary | 151
- Page 154 and 155: problems in both locomotor skills a
- Page 156 and 157: subjects are to be applied to perso
- Page 158 and 159: may be an indicator of activity lev
- Page 160 and 161: SamenvattingSamenvatting | 159
- Page 162 and 163: InleidingVoldoende bewegen en fithe
- Page 164 and 165: verstandelijk niveau en bepaalde mo
- Page 166 and 167: Hieruit bleek, dat de motivatie van
- Page 168 and 169: Verder is duidelijk geworden dat me
- Page 170 and 171: DankwoordDankwoord | 169
- Page 172 and 173: De leden van de leescommissie, prof
- Page 174 and 175: Judith van der Boom, dank je wel vo
- Page 176 and 177:
Dankwoord | 175
- Page 178 and 179:
Curriculum vitaeCurriculum vitae |
- Page 180:
Curriculum vitae | 179