studies. Randomized Controlled Trials (RCT’s) are considered to be the most reliable and valid wayto perform <strong>in</strong>tervention studies <strong>in</strong> various populations. Comparison between groups is thought toreflect differences <strong>in</strong> effect of the <strong>in</strong>terventions. The required sample size <strong>in</strong> RCT’s depends partlyon the variation between participants: a large variation calls for a larger sample size. Therefore,many studies <strong>in</strong>clude homogeneous groups. However, due to the variety of their co-morbidities,it is difficult to compose a homogeneous study population <strong>with</strong> sufficient power composedof persons <strong>with</strong> SPIMD. Neither is it possible to compose a large heterogeneous SPIMD studypopulation. As a consequence, both the experimental and control group will consist of participants<strong>with</strong> much variation <strong>in</strong> their co-morbidities, result<strong>in</strong>g <strong>in</strong> a wide array of responses to the same<strong>in</strong>tervention. In such circumstances detect<strong>in</strong>g significant effects of an <strong>in</strong>tervention is ratherdifficult. An anecdote from practical experience will illustrate this.To subject three participants <strong>with</strong> SPIMD to passive or assistive active movements, poweredexercise equipment (Shapemaster®, Barth Fidder, Shapemaster Benelux) was used. Thesemach<strong>in</strong>es are fitted <strong>with</strong> motors and gearboxes, and controlled by microchip technology. Themach<strong>in</strong>es automatically move selected levers and handles at pre-determ<strong>in</strong>ed speeds through apre-determ<strong>in</strong>ed range of motion. Each mach<strong>in</strong>e provides multi-function movements. The outcomemeasures are bodycomposition, muscle tone, heart rate, oxygen saturation and alertness [39]. Atthe <strong>in</strong>dividual level, relevant improvements were found for the different outcome measures.1. A woman of 38 years old, <strong>with</strong> profound ID, GMFCS level IV, no spasticity, totally bl<strong>in</strong>d,epilepsy, and be<strong>in</strong>g overweight, participated <strong>in</strong> the study. Her BMI before the <strong>in</strong>terventionwas 27.7 kg/cm 2 , after the <strong>in</strong>tervention 26.2 kg/cm 2 , which means a difference of 1.5 kg/cm 2 .Her waist circumference decreases from 89 cm, which means abdom<strong>in</strong>al obesitas, to 83 cm,which is <strong>in</strong>dicat<strong>in</strong>g ‘healthy weight but attention needed’ [7]. Oxygen saturation dur<strong>in</strong>g andafter mov<strong>in</strong>g on the mach<strong>in</strong>es <strong>in</strong>creased from 95% before the <strong>in</strong>tervention program, to 99 %after 20 weeks. However, muscle tone, alertness and hart frequency showed no differences.2. A girl of 17 years old, <strong>with</strong> profound ID, GMFCS level V, severe partially sighted, <strong>with</strong>spasticity, epilepsy and orthopedic defects also participated <strong>in</strong> the study. Her muscle tone<strong>in</strong> the legs decreased <strong>in</strong> 20 weeks <strong>with</strong> two po<strong>in</strong>ts on the six po<strong>in</strong>t scale of the ModifiedAshworth Scale. After every <strong>in</strong>crease <strong>in</strong> <strong>in</strong>tensity <strong>in</strong> a five weeks period, her heart rate<strong>in</strong>creased first one or two heart rate zones dur<strong>in</strong>g mov<strong>in</strong>g, but after three weeks, heart ratedecreased aga<strong>in</strong> to the first level. This might <strong>in</strong>dicate a tra<strong>in</strong><strong>in</strong>g effect. However, saturation,alertness, BMI and waist circumference showed no differences.3. A man of 43 years old, <strong>with</strong> profound ID, GMFCS level V, totally bl<strong>in</strong>d, spasticity, epilepsy,and orthopedic defects, also participated <strong>in</strong> the study. His muscle tone <strong>in</strong> both arms andlegs decreased <strong>in</strong> 20 weeks <strong>with</strong> one po<strong>in</strong>t on the six po<strong>in</strong>t scale of the Modified AshworthScale. Oxygen saturation dur<strong>in</strong>g mov<strong>in</strong>g on the mach<strong>in</strong>es <strong>in</strong>creased from 91% before the<strong>in</strong>tervention program, to 95 % after 20 weeks. BMI decreased after the <strong>in</strong>tervention <strong>with</strong>0.5 kg/cm 2 , but before and after the <strong>in</strong>tervention he already had a healthy BMI. Alertness<strong>in</strong>creased dur<strong>in</strong>g <strong>in</strong>tervention <strong>with</strong> one po<strong>in</strong>t on a four po<strong>in</strong>t scale [39]. However, heart rateshowed no differences dur<strong>in</strong>g and after the <strong>in</strong>tervention period.As shown, <strong>in</strong>dividuals benefit from the <strong>in</strong>tervention but not <strong>in</strong> the same way nor to the sameextent. Individual differences <strong>in</strong> characteristics of locomotor skills, visual impairment, comorbidities,and basel<strong>in</strong>e measurements of the outcome measures account for this result. Yet,there were benefits, albeit different ones for different subjects. In group comparison studies therelevant <strong>in</strong>dividual benefits can be overlooked. Consequently, next to traditional research designs,Chapter 9 | 145
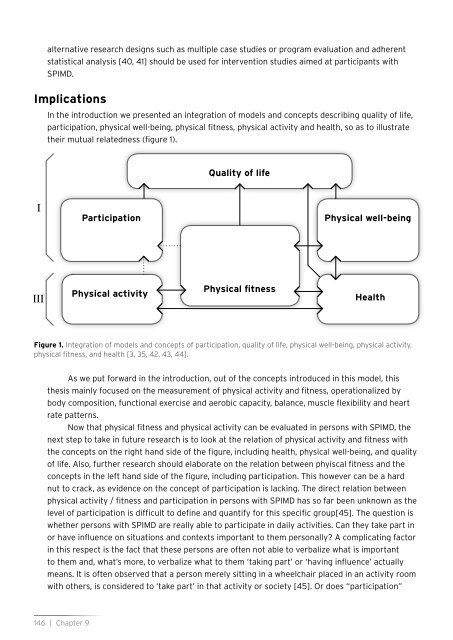
alternative research designs such as multiple case studies or program evaluation and adherentstatistical analysis [40, 41] should be used for <strong>in</strong>tervention studies aimed at participants <strong>with</strong>SPIMD.ImplicationsIn the <strong>in</strong>troduction we presented an <strong>in</strong>tegration of models and concepts describ<strong>in</strong>g quality of life,participation, <strong>physical</strong> well-be<strong>in</strong>g, <strong>physical</strong> <strong>fitness</strong>, <strong>physical</strong> activity and health, so as to illustratetheir mutual relatedness (figure 1).Quality of lifeIParticipationPhysical well-be<strong>in</strong>gIIIPhysical activityPhysical <strong>fitness</strong>HealthFigure 1. Integration of models and concepts of participation, quality of life, <strong>physical</strong> well-be<strong>in</strong>g, <strong>physical</strong> activity,<strong>physical</strong> <strong>fitness</strong>, and health [3, 35, 42, 43, 44].As we put forward <strong>in</strong> the <strong>in</strong>troduction, out of the concepts <strong>in</strong>troduced <strong>in</strong> this model, thisthesis ma<strong>in</strong>ly focused on the measurement of <strong>physical</strong> activity and <strong>fitness</strong>, operationalized bybody composition, functional exercise and aerobic capacity, balance, muscle flexibility and heartrate patterns.Now that <strong>physical</strong> <strong>fitness</strong> and <strong>physical</strong> activity can be evaluated <strong>in</strong> persons <strong>with</strong> SPIMD, thenext step to take <strong>in</strong> future research is to look at the relation of <strong>physical</strong> activity and <strong>fitness</strong> <strong>with</strong>the concepts on the right hand side of the figure, <strong>in</strong>clud<strong>in</strong>g health, <strong>physical</strong> well-be<strong>in</strong>g, and qualityof life. Also, further research should elaborate on the relation between phyiscal <strong>fitness</strong> and theconcepts <strong>in</strong> the left hand side of the figure, <strong>in</strong>clud<strong>in</strong>g participation. This however can be a hardnut to crack, as evidence on the concept of participation is lack<strong>in</strong>g. The direct relation between<strong>physical</strong> activity / <strong>fitness</strong> and participation <strong>in</strong> persons <strong>with</strong> SPIMD has so far been unknown as thelevel of participation is difficult to def<strong>in</strong>e and quantify for this specific group[45]. The question iswhether persons <strong>with</strong> SPIMD are really able to participate <strong>in</strong> daily activities. Can they take part <strong>in</strong>or have <strong>in</strong>fluence on situations and contexts important to them personally? A complicat<strong>in</strong>g factor<strong>in</strong> this respect is the fact that these persons are often not able to verbalize what is importantto them and, what’s more, to verbalize what to them ‘tak<strong>in</strong>g part’ or ‘hav<strong>in</strong>g <strong>in</strong>fluence’ actuallymeans. It is often observed that a person merely sitt<strong>in</strong>g <strong>in</strong> a wheelchair placed <strong>in</strong> an activity room<strong>with</strong> others, is considered to ‘take part’ <strong>in</strong> that activity or society [45]. Or does “participation”146 | Chapter 9
- Page 2 and 3:
Measuring physical fitnessin person
- Page 4:
Rijksuniversiteit GroningenMeasurin
- Page 10 and 11:
Chapter 1IntroductionChapter 1 | 9
- Page 12 and 13:
overweight [15]. This prevalence is
- Page 14 and 15:
Theoretical framework of the studyI
- Page 16 and 17:
Components of physical fitnessThe a
- Page 18 and 19:
Therefore, a study is put forward w
- Page 20 and 21:
2002;40:436-444.19 Temple VA, Frey
- Page 22 and 23:
Chapter 2Feasibility and reliabilit
- Page 24 and 25:
IntroductionPhysical fitness and he
- Page 26 and 27:
GMFCS was presented to the investig
- Page 28 and 29:
Body weightTo determine the body we
- Page 30 and 31:
Table 1 Results of Wilcoxon rank te
- Page 32 and 33:
Calculation of heightThe mean (SD)
- Page 34 and 35:
DiscussionThe results of our study
- Page 36 and 37:
References1 Bouchard C, Shepard RJ,
- Page 38 and 39:
37 Rimmer J, Kelly LE, Rosentswieg
- Page 40 and 41:
Chapter 3Measuring waist circumfere
- Page 42 and 43:
IntroductionChildren and adults wit
- Page 44 and 45:
participants. These calculations as
- Page 46 and 47:
Data analysisThe data were analyzed
- Page 48:
Table 2. Simple regression analysis
- Page 54 and 55:
Chapter 4Feasibility and reliabilit
- Page 56 and 57:
IntroductionPeople with intellectua
- Page 58 and 59:
Eighty representatives gave permiss
- Page 60 and 61:
3) The measurement procedure: The m
- Page 62 and 63:
and whether motivation influenced t
- Page 64 and 65:
Table 3. Mean peak heart rate achie
- Page 66 and 67:
AcknowledgementsThis research was f
- Page 68 and 69:
21 Hopkins WG, Gaeta H, Thomas AC,
- Page 70 and 71:
Chapter 5Psychometric quality of a
- Page 72 and 73:
IntroductionIntellectual disability
- Page 74 and 75:
Exclusion criteria were mental or p
- Page 76 and 77:
participant had fulfilled the task.
- Page 78 and 79:
Table 2. Descriptive results peak h
- Page 80 and 81:
Table 3. Test-retest reliability of
- Page 82 and 83:
Table 4. Correlation scored motivat
- Page 84 and 85:
preceding GXT results on HR peak. G
- Page 86 and 87:
References1 Schalock R, Brown I, Br
- Page 88 and 89:
37 Stanish HI, Temple VA, Frey GC.
- Page 90 and 91:
Chapter 6Feasibility and reliabilit
- Page 92 and 93:
IntroductionLocomotor skills in peo
- Page 94 and 95:
this study was to evaluate the feas
- Page 96 and 97: obtained from the legal representat
- Page 98 and 99: Modified Berg Balance Scale scoresI
- Page 100 and 101: Modified Berg Balance Scale scoresT
- Page 102 and 103: References1 Van Erkelens-Zwets JHJ
- Page 104 and 105: 39 Dorai-Raj S. Binomial Confidence
- Page 106 and 107: Chapter 7Feasibility, test-retest r
- Page 108 and 109: IntroductionPersons with profound i
- Page 110 and 111: DesignThe muscle tone and spasticit
- Page 112 and 113: Interrater reliabilityFirstly, to d
- Page 114 and 115: Table 3. Summary of the statistical
- Page 116 and 117: Table 6. Summary of the statistical
- Page 118 and 119: RecommendationsThe feasibility of c
- Page 120 and 121: 18 Gielen EJJM. Is spasticiteit te
- Page 122 and 123: Chapter 8Heart Rate Pattern as an I
- Page 124 and 125: IntroductionIt is important to gain
- Page 126 and 127: 48 persons18 persons lacked permiss
- Page 128 and 129: Furthermore, the mean and the range
- Page 130 and 131: Table 3. Day-to-day outline of the
- Page 132 and 133: Relation between heart rate pattern
- Page 134 and 135: patterns in this study we can concl
- Page 136 and 137: References1 Emerson E. Underweight,
- Page 138 and 139: 38 Multilevel Models Project (2004)
- Page 140 and 141: Chapter 9General DiscussionChapter
- Page 142 and 143: on this. To sum up, testing in pers
- Page 144 and 145: for future research it is recommend
- Page 148 and 149: of these individuals require more?
- Page 150 and 151: 19 Lahtinen U, Rintala P, Malin A.
- Page 152 and 153: SummarySummary | 151
- Page 154 and 155: problems in both locomotor skills a
- Page 156 and 157: subjects are to be applied to perso
- Page 158 and 159: may be an indicator of activity lev
- Page 160 and 161: SamenvattingSamenvatting | 159
- Page 162 and 163: InleidingVoldoende bewegen en fithe
- Page 164 and 165: verstandelijk niveau en bepaalde mo
- Page 166 and 167: Hieruit bleek, dat de motivatie van
- Page 168 and 169: Verder is duidelijk geworden dat me
- Page 170 and 171: DankwoordDankwoord | 169
- Page 172 and 173: De leden van de leescommissie, prof
- Page 174 and 175: Judith van der Boom, dank je wel vo
- Page 176 and 177: Dankwoord | 175
- Page 178 and 179: Curriculum vitaeCurriculum vitae |
- Page 180: Curriculum vitae | 179