Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
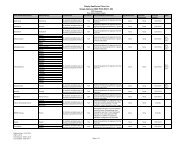
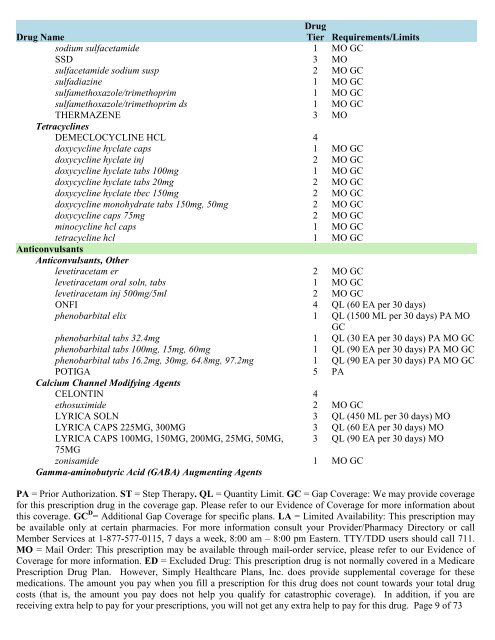
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/Limitssodium sulfacetamide 1 MO GCSSD 3 MOsulfacetamide sodium susp 2 MO GCsulfadiazine 1 MO GCsulfamethoxazole/trimethoprim 1 MO GCsulfamethoxazole/trimethoprim ds 1 MO GCTHERMAZENE 3 MOTetracyclinesDEMECLOCYCLINE HCL 4doxycycline hyclate caps 1 MO GCdoxycycline hyclate inj 2 MO GCdoxycycline hyclate tabs 100mg 1 MO GCdoxycycline hyclate tabs 20mg 2 MO GCdoxycycline hyclate tbec 150mg 2 MO GCdoxycycline monohydrate tabs 150mg, 50mg 2 MO GCdoxycycline caps 75mg 2 MO GCminocycline hcl caps 1 MO GCtetracycline hcl 1 MO GCAnticonvulsantsAnticonvulsants, Otherlevetiracetam er 2 MO GClevetiracetam oral soln, tabs 1 MO GClevetiracetam inj 500mg/5ml 2 MO GCONFI 4 QL (60 EA per 30 days)phenobarbital elix 1 QL (1500 ML per 30 days) PA MOGCphenobarbital tabs 32.4mg 1 QL (30 EA per 30 days) PA MO GCphenobarbital tabs 100mg, 15mg, 60mg 1 QL (90 EA per 30 days) PA MO GCphenobarbital tabs 16.2mg, 30mg, 64.8mg, 97.2mg 1 QL (90 EA per 30 days) PA MO GCPOTIGA 5 PACalcium Channel Modifying AgentsCELONTIN 4ethosuximide 2 MO GCLYRICA SOLN 3 QL (450 ML per 30 days) MOLYRICA CAPS 225MG, 300MG 3 QL (60 EA per 30 days) MOLYRICA CAPS 100MG, 150MG, 200MG, 25MG, 50MG, 3 QL (90 EA per 30 days) MO75MGzonisamide 1 MO GCGamma-aminobutyric Acid (GABA) Augmenting AgentsPA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. GC D = Additional Gap Coverage for specific plans. LA = Limited Availability: This prescription maybe available only at certain pharmacies. For more information consult your Provider/Pharmacy Directory or callMember Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711.MO = Mail Order: This prescription may be available through mail-order service, please refer to our Evidence <strong>of</strong>Coverage for more information. ED = Excluded <strong>Drug</strong>: This prescription drug is not normally <strong>covered</strong> in a Medicare<strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans, Inc. does provide supplemental coverage for thesemedications. The amount you pay when you fill a prescription for this drug does not count towards your total drugcosts (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you arereceiving extra help to pay for your prescriptions, you will not get any extra help to pay for this drug. Page 9 <strong>of</strong> 73