Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
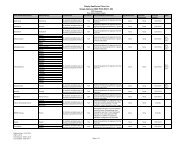
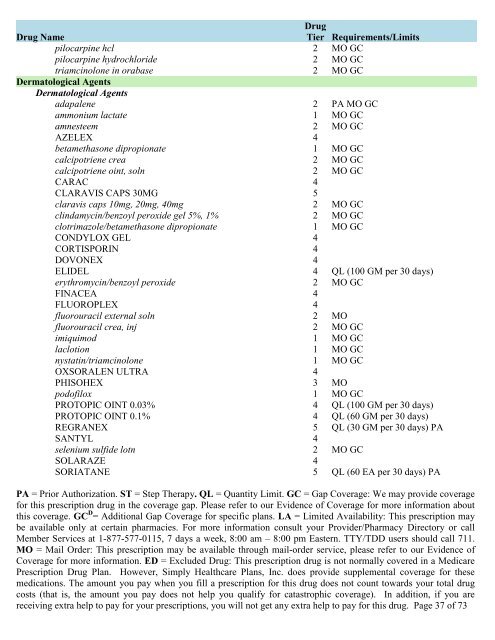
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/Limitspilocarpine hcl 2 MO GCpilocarpine hydrochloride 2 MO GCtriamcinolone in orabase 2 MO GCDermatological AgentsDermatological Agentsadapalene 2 PA MO GCammonium lactate 1 MO GCamnesteem 2 MO GCAZELEX 4betamethasone dipropionate 1 MO GCcalcipotriene crea 2 MO GCcalcipotriene oint, soln 2 MO GCCARAC 4CLARAVIS CAPS 30MG 5claravis caps 10mg, 20mg, 40mg 2 MO GCclindamycin/benzoyl peroxide gel 5%, 1% 2 MO GCclotrimazole/betamethasone dipropionate 1 MO GCCONDYLOX GEL 4CORTISPORIN 4DOVONEX 4ELIDEL 4 QL (100 GM per 30 days)erythromycin/benzoyl peroxide 2 MO GCFINACEA 4FLUOROPLEX 4fluorouracil external soln 2 MOfluorouracil crea, inj 2 MO GCimiquimod 1 MO GClaclotion 1 MO GCnystatin/triamcinolone 1 MO GCOXSORALEN ULTRA 4PHISOHEX 3 MOpod<strong>of</strong>ilox 1 MO GCPROTOPIC OINT 0.03% 4 QL (100 GM per 30 days)PROTOPIC OINT 0.1% 4 QL (60 GM per 30 days)REGRANEX 5 QL (30 GM per 30 days) PASANTYL 4selenium sulfide lotn 2 MO GCSOLARAZE 4SORIATANE 5 QL (60 EA per 30 days) PAPA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. GC D = Additional Gap Coverage for specific plans. LA = Limited Availability: This prescription maybe available only at certain pharmacies. For more information consult your Provider/Pharmacy Directory or callMember Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711.MO = Mail Order: This prescription may be available through mail-order service, please refer to our Evidence <strong>of</strong>Coverage for more information. ED = Excluded <strong>Drug</strong>: This prescription drug is not normally <strong>covered</strong> in a Medicare<strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans, Inc. does provide supplemental coverage for thesemedications. The amount you pay when you fill a prescription for this drug does not count towards your total drugcosts (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you arereceiving extra help to pay for your prescriptions, you will not get any extra help to pay for this drug. Page 37 <strong>of</strong> 73