Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
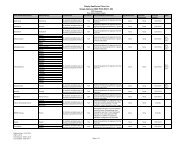
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/LimitsCAPRELSA TABS 300MG 5 QL (90 EA per 90 days) PA LAGLEEVEC TABS 400MG 5 QL (60 EA per 30 days) PAGLEEVEC TABS 100MG 5 QL (90 EA per 30 days) PANEXAVAR 5 QL (120 EA per 30 days) PA LASPRYCEL TABS 20MG 5 QL (150 EA per 30 days) PASPRYCEL TABS 140MG, 80MG 5 QL (30 EA per 30 days) PASPRYCEL TABS 100MG, 50MG, 70MG 5 QL (60 EA per 30 days) PASUTENT CAPS 25MG, 50MG 5 QL (30 EA per 30 days) PASUTENT CAPS 12.5MG 5 QL (90 EA per 30 days) PATARCEVA TABS 25MG 5 QL (60 EA per 30 days) PATARCEVA TABS 100MG, 150MG 5 QL (90 EA per 90 days) PATASIGNA 5 QL (120 EA per 30 days) PATYKERB 5 QL (540 EA per 90 days) PA LAVOTRIENT 5 QL (360 EA per 90 days) PAXALKORI 5 QL (60 EA per 30 days) PAMonoclonal AntibodiesARZERRA INJ 100MG/5ML 5 PARITUXAN 5 PARetinoidsPANRETIN 5 PATARGRETIN 5 PATRETINOIN CAPS 3 MOtretinoin crea, gel 2 PA MO GCAntiparasiticsAnthelminticsALBENZA 3 MOBILTRICIDE 3 MOSTROMECTOL 3 MOAntiprotozoalsALINIA TABS 4atovaquone/proguanil hcl tabs 250mg, 100mg 2 MO GCchloroquine phosphate 1 MO GCDARAPRIM 4hydroxychloroquine sulfate 1 MO GCmefloquine hcl 2 MO GCMEPRON 5NEBUPENT 4 B/DQUALAQUIN 4 QL (42 EA per 30 days)quinine sulfate 2 MO GCPA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. GC D = Additional Gap Coverage for specific plans. LA = Limited Availability: This prescription maybe available only at certain pharmacies. For more information consult your Provider/Pharmacy Directory or callMember Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711.MO = Mail Order: This prescription may be available through mail-order service, please refer to our Evidence <strong>of</strong>Coverage for more information. ED = Excluded <strong>Drug</strong>: This prescription drug is not normally <strong>covered</strong> in a Medicare<strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans, Inc. does provide supplemental coverage for thesemedications. The amount you pay when you fill a prescription for this drug does not count towards your total drugcosts (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you arereceiving extra help to pay for your prescriptions, you will not get any extra help to pay for this drug. Page 19 <strong>of</strong> 73