Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs
Prescription Drug Guide Comprehensive list of covered drugs

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
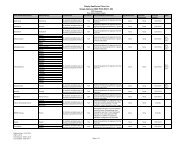
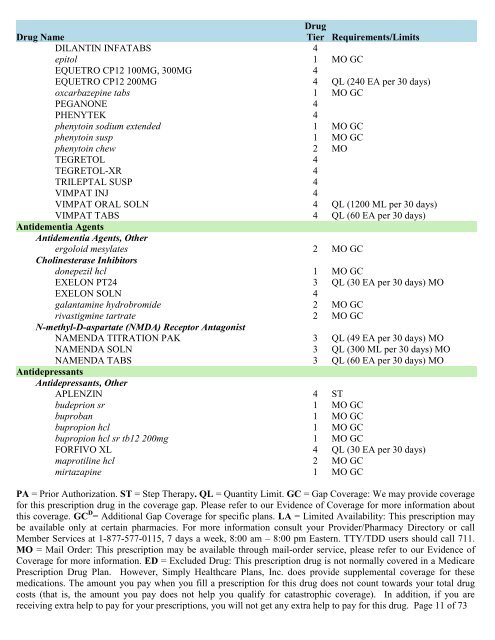
<strong>Drug</strong> Name<strong>Drug</strong>Tier Requirements/LimitsDILANTIN INFATABS 4epitol 1 MO GCEQUETRO CP12 100MG, 300MG 4EQUETRO CP12 200MG 4 QL (240 EA per 30 days)oxcarbazepine tabs 1 MO GCPEGANONE 4PHENYTEK 4phenytoin sodium extended 1 MO GCphenytoin susp 1 MO GCphenytoin chew 2 MOTEGRETOL 4TEGRETOL-XR 4TRILEPTAL SUSP 4VIMPAT INJ 4VIMPAT ORAL SOLN 4 QL (1200 ML per 30 days)VIMPAT TABS 4 QL (60 EA per 30 days)Antidementia AgentsAntidementia Agents, Otherergoloid mesylates 2 MO GCCholinesterase Inhibitorsdonepezil hcl 1 MO GCEXELON PT24 3 QL (30 EA per 30 days) MOEXELON SOLN 4galantamine hydrobromide 2 MO GCrivastigmine tartrate 2 MO GCN-methyl-D-aspartate (NMDA) Receptor AntagonistNAMENDA TITRATION PAK 3 QL (49 EA per 30 days) MONAMENDA SOLN 3 QL (300 ML per 30 days) MONAMENDA TABS 3 QL (60 EA per 30 days) MOAntidepressantsAntidepressants, OtherAPLENZIN 4 STbudeprion sr 1 MO GCbuproban 1 MO GCbupropion hcl 1 MO GCbupropion hcl sr tb12 200mg 1 MO GCFORFIVO XL 4 QL (30 EA per 30 days)maprotiline hcl 2 MO GCmirtazapine 1 MO GCPA = Prior Authorization. ST = Step Therapy. QL = Quantity Limit. GC = Gap Coverage: We may provide coveragefor this prescription drug in the coverage gap. Please refer to our Evidence <strong>of</strong> Coverage for more information aboutthis coverage. GC D = Additional Gap Coverage for specific plans. LA = Limited Availability: This prescription maybe available only at certain pharmacies. For more information consult your Provider/Pharmacy Directory or callMember Services at 1-877-577-0115, 7 days a week, 8:00 am – 8:00 pm Eastern. TTY/TDD users should call 711.MO = Mail Order: This prescription may be available through mail-order service, please refer to our Evidence <strong>of</strong>Coverage for more information. ED = Excluded <strong>Drug</strong>: This prescription drug is not normally <strong>covered</strong> in a Medicare<strong>Prescription</strong> <strong>Drug</strong> Plan. However, Simply Healthcare Plans, Inc. does provide supplemental coverage for thesemedications. The amount you pay when you fill a prescription for this drug does not count towards your total drugcosts (that is, the amount you pay does not help you qualify for catastrophic coverage). In addition, if you arereceiving extra help to pay for your prescriptions, you will not get any extra help to pay for this drug. Page 11 <strong>of</strong> 73