EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
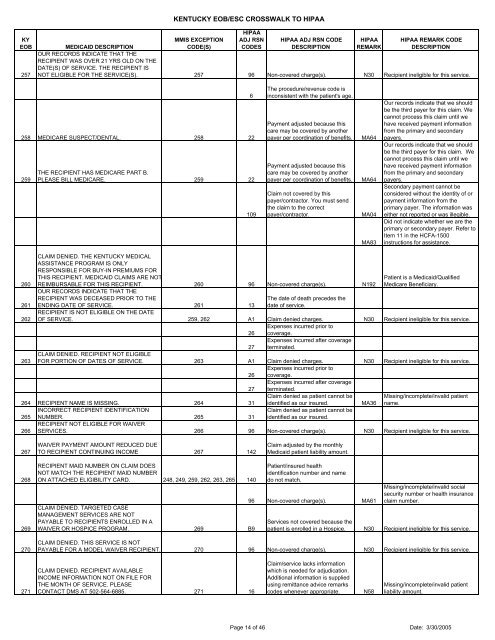
KY<strong>EOB</strong>257KENTUCKY <strong>EOB</strong>/ESC CROSSWALK TO HIPAAMMIS EXCEPTIONCODE(S)HIPAAADJ RSNCODESHIPAA ADJ RSN CODEDESCRIPTIONHIPAAREMARKHIPAA REMARK CODEDESCRIPTIONMEDICAID DESCRIPTIONOUR RECORDS INDICATE THAT THERECIPIENT WAS OVER 21 YRS OLD ON THEDATE(S) OF SERVICE. THE RECIPIENT ISNOT ELIGIBLE FOR THE SERVICE(S). 257 96 Non-covered charge(s). N30 Recipient ineligible for this service.258 MEDICARE SUSPECT/DENTAL. 258 22259THE RECIPIENT HAS MEDICARE PART B.PLEASE BILL MEDICARE. 259 226109The procedure/revenue code isinconsistent with the patient's age.Payment adjusted because thiscare may be covered by anotherpayer per coordination of benefits.Payment adjusted because thiscare may be covered by anotherpayer per coordination of benefits.Claim not covered by thispayer/contractor. You must sendthe claim to the correctpayer/contractor.MA64MA64MA04MA83Our records indicate that we shouldbe the third payer for this claim. Wecannot process this claim until wehave received payment informationfrom the primary <strong>and</strong> secondarypayers.Our records indicate that we shouldbe the third payer for this claim. Wecannot process this claim until wehave received payment informationfrom the primary <strong>and</strong> secondarypayers.Secondary payment cannot beconsidered without the identity of orpayment information from theprimary payer. The information waseither not reported or was illegible.Did not indicate whether we are theprimary or secondary payer. Refer toItem 11 in the HCFA-1500instructions for assistance.260261CLAIM DENIED. THE KENTUCKY MEDICALASSISTANCE PROGRAM IS ONLYRESPONSIBLE FOR BUY-IN PREMIUMS FORTHIS RECIPIENT. MEDICAID CLAIMS ARE NOTREIMBURSABLE FOR THIS RECIPIENT. 260 96 Non-covered charge(s). N192OUR RECORDS INDICATE THAT THERECIPIENT WAS DECEASED PRIOR TO THEENDING DATE OF SERVICE. 261 13RECIPIENT IS NOT ELIGIBLE ON THE DATEThe date of death precedes thedate of service.Patient is a Medicaid/QualifiedMedicare Beneficiary.262 OF SERVICE. 259, 262 A1 Claim denied charges. N30 Recipient ineligible for this service.Expenses incurred prior to26 coverage.Expenses incurred after coverage27 terminated.CLAIM DENIED. RECIPIENT NOT ELIGIBLE263 FOR PORTION OF DATES OF SERVICE. 263 A1 Claim denied charges. N30 Recipient ineligible for this service.Expenses incurred prior to26 coverage.Expenses incurred after coverage27 terminated.Claim denied as patient cannot beMissing/in<strong>com</strong>plete/invalid patient264 RECIPIENT NAME IS MISSING. 264 31 identified as our insured.MA36 name.INCORRECT RECIPIENT IDENTIFICATIONClaim denied as patient cannot be265 NUMBER. 265 31 identified as our insured.RECIPIENT NOT ELIGIBLE FOR WAIVER266 SERVICES. 266 96 Non-covered charge(s). N30 Recipient ineligible for this service.267WAIVER PAYMENT AMOUNT REDUCED DUETO RECIPIENT CONTINUING INCOME 267 142Claim adjusted by the monthlyMedicaid patient liability amount.268269270RECIPIENT MAID NUMBER ON CLAIM DOESNOT MATCH THE RECIPIENT MAID NUMBERON ATTACHED ELIGIBILITY CARD. 248, 249, 259, 262, 263, 265 140CLAIM DENIED. TARGETED CASEMANAGEMENT SERVICES ARE NOTPAYABLE TO RECIPIENTS ENROLLED IN AWAIVER OR HOSPICE PROGRAM. 269 B9Patient/insured healthidentification number <strong>and</strong> namedo not match.96 Non-covered charge(s). MA61Missing/in<strong>com</strong>plete/invalid socialsecurity number or health insuranceclaim number.Services not covered because thepatient is enrolled in a Hospice. N30 Recipient ineligible for this service.CLAIM DENIED. THIS SERVICE IS NOTPAYABLE FOR A MODEL WAIVER RECIPIENT. 270 96 Non-covered charge(s). N30 Recipient ineligible for this service.271CLAIM DENIED. RECIPIENT AVAILABLEINCOME INFORMATION NOT ON FILE FORTHE MONTH OF SERVICE. PLEASECONTACT DMS AT 502-564-6885. 271 16Claim/service lacks informationwhich is needed for adjudication.Additional information is suppliedusing remittance advice remarkscodes whenever appropriate.N58Missing/in<strong>com</strong>plete/invalid patientliability amount.Page 14 of 46 Date: 3/30/2005