EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
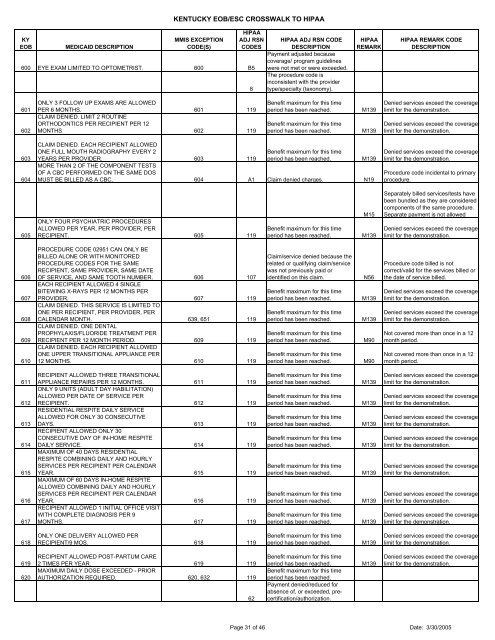
KY<strong>EOB</strong>MEDICAID DESCRIPTIONKENTUCKY <strong>EOB</strong>/ESC CROSSWALK TO HIPAAMMIS EXCEPTIONCODE(S)HIPAAADJ RSNCODES600 EYE EXAM LIMITED TO OPTOMETRIST. 600 B58HIPAA ADJ RSN CODEDESCRIPTIONPayment adjusted becausecoverage/ program guidelineswere not met or were exceeded.The procedure code isinconsistent with the providertype/specialty (taxonomy).HIPAAREMARKHIPAA REMARK CODEDESCRIPTION601602ONLY 3 FOLLOW UP EXAMS ARE ALLOWEDPER 6 MONTHS. 601 119CLAIM DENIED. LIMIT 2 ROUTINEORTHODONTICS PER RECIPIENT PER 12MONTHS 602 119Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.M139M139Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.603604CLAIM DENIED. EACH RECIPIENT ALLOWEDONE FULL MOUTH RADIOGRAPHY EVERY 2YEARS PER PROVIDER. 603 119Benefit maximum for this timeperiod has been reached.M139MORE THAN 2 OF THE COMPONENT TESTSOF A CBC PERFORMED ON THE SAME DOSMUST BE BILLED AS A CBC. 604 A1 Claim denied charges. N19Denied services exceed the coveragelimit for the demonstration.Procedure code incidental to primaryprocedure.605ONLY FOUR PSYCHIATRIC PROCEDURESALLOWED PER YEAR, PER PROVIDER, PERRECIPIENT. 605 119Benefit maximum for this timeperiod has been reached.M15M139Separately billed services/tests havebeen bundled as they are considered<strong>com</strong>ponents of the same procedure.Separate payment is not allowedDenied services exceed the coveragelimit for the demonstration.606607608609610PROCEDURE CODE 02951 CAN ONLY BEBILLED ALONE OR WITH MONITOREDPROCEDURE CODES FOR THE SAMERECIPIENT, SAME PROVIDER, SAME DATEOF SERVICE, AND SAME TOOTH NUMBER. 606 107EACH RECIPIENT ALLOWED 4 SINGLEBITEWING X-RAYS PER 12 MONTHS PERPROVIDER. 607 119CLAIM DENIED. THIS SERVICE IS LIMITED TOONE PER RECIPIENT, PER PROVIDER, PERCALENDAR MONTH. 639, 651 119CLAIM DENIED. ONE DENTALPROPHYLAXIS/FLUORIDE TREATMENT PERRECIPIENT PER 12 MONTH PERIOD. 609 119CLAIM DENIED. EACH RECIPIENT ALLOWEDONE UPPER TRANSITIONAL APPLIANCE PER12 MONTHS. 610 119Claim/service denied because therelated or qualifying claim/servicewas not previously paid oridentified on this claim.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.N56M139M139M90M90Procedure code billed is notcorrect/valid for the services billed orthe date of service billed.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Not covered more than once in a 12month period.Not covered more than once in a 12month period.611612613614615616617RECIPIENT ALLOWED THREE TRANSITIONALAPPLIANCE REPAIRS PER 12 MONTHS. 611 119ONLY 9 UNITS (ADULT DAY HABILITATION)ALLOWED PER DATE OF SERVICE PERRECIPIENT. 612 119RESIDENTIAL RESPITE DAILY SERVICEALLOWED FOR ONLY 30 CONSECUTIVEDAYS. 613 119RECIPIENT ALLOWED ONLY 30CONSECUTIVE DAY OF IN-HOME RESPITEDAILY SERVICE. 614 119MAXIMUM OF 40 DAYS RESIDENTIALRESPITE COMBINING DAILY AND HOURLYSERVICES PER RECIPIENT PER CALENDARYEAR. 615 119MAXIMUM OF 60 DAYS IN-HOME RESPITEALLOWED COMBINING DAILY AND HOURLYSERVICES PER RECIPIENT PER CALENDARYEAR. 616 119RECIPIENT ALLOWED 1 INITIAL OFFICE VISITWITH COMPLETE DIAGNOSIS PER 9MONTHS. 617 119Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.M139M139M139M139M139M139M139Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.Denied services exceed the coveragelimit for the demonstration.618ONLY ONE DELIVERY ALLOWED PERRECIPIENT/9 MOS. 618 119Benefit maximum for this timeperiod has been reached.M139Denied services exceed the coveragelimit for the demonstration.619620RECIPIENT ALLOWED POST-PARTUM CARE2 TIMES PER YEAR. 619 119MAXIMUM DAILY DOSE EXCEEDED - PRIORAUTHORIZATION REQUIRED. 620, 632 11962Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Payment denied/reduced forabsence of, or exceeded, precertification/authorization.M139Denied services exceed the coveragelimit for the demonstration.Page 31 of 46 Date: 3/30/2005