EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
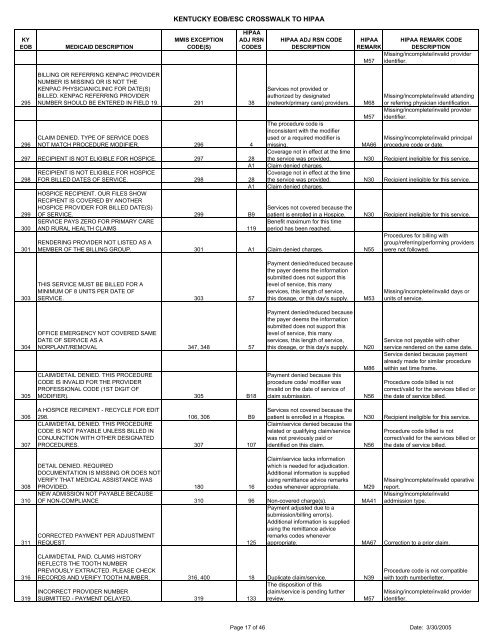
KENTUCKY <strong>EOB</strong>/ESC CROSSWALK TO HIPAAKY<strong>EOB</strong>MEDICAID DESCRIPTIONMMIS EXCEPTIONCODE(S)HIPAAADJ RSNCODESHIPAA ADJ RSN CODEDESCRIPTIONHIPAA HIPAA REMARK CODEREMARKDESCRIPTIONMissing/in<strong>com</strong>plete/invalid providerM57 identifier.295296BILLING OR REFERRING KENPAC PROVIDERNUMBER IS MISSING OR IS NOT THEKENPAC PHYSICIAN/CLINIC FOR DATE(S)BILLED. KENPAC REFERRING PROVIDERNUMBER SHOULD BE ENTERED IN FIELD 19. 291 38CLAIM DENIED. TYPE OF SERVICE DOESNOT MATCH PROCEDURE MODIFIER. 296 4297 RECIPIENT IS NOT ELIGIBLE FOR HOSPICE. 297 28A1RECIPIENT IS NOT ELIGIBLE FOR HOSPICE298 FOR BILLED DATES OF SERVICE. 298 28A1HOSPICE RECIPIENT. OUR FILES SHOWRECIPIENT IS COVERED BY ANOTHERHOSPICE PROVIDER FOR BILLED DATE(S)299 OF SERVICE. 299 B9SERVICE PAYS ZERO FOR PRIMARY CARE300 AND RURAL HEALTH CLAIMS 119301Services not provided orauthorized by designated(network/primary care) providers.The procedure code isinconsistent with the modifierused or a required modifier ismissing.Coverage not in effect at the timeM68M57MA66Missing/in<strong>com</strong>plete/invalid attendingor referring physician identification.Missing/in<strong>com</strong>plete/invalid provideridentifier.Missing/in<strong>com</strong>plete/invalid principalprocedure code or date.the service was provided. N30 Recipient ineligible for this service.Claim denied charges.Coverage not in effect at the timethe service was provided. N30 Recipient ineligible for this service.Claim denied charges.Services not covered because thepatient is enrolled in a Hospice. N30 Recipient ineligible for this service.Benefit maximum for this timeperiod has been reached.Procedures for billing withgroup/referring/performing providerswere not followed.RENDERING PROVIDER NOT LISTED AS AMEMBER OF THE BILLING GROUP. 301 A1 Claim denied charges. N55303THIS SERVICE MUST BE BILLED FOR AMINIMUM OF 8 UNITS PER DATE OFSERVICE. 303 57Payment denied/reduced becausethe payer deems the informationsubmitted does not support thislevel of service, this manyservices, this length of service,this dosage, or this day's supply.M53Missing/in<strong>com</strong>plete/invalid days orunits of service.304305OFFICE EMERGENCY NOT COVERED SAMEDATE OF SERVICE AS ANORPLANT/REMOVAL 347, 348 57CLAIM/DETAIL DENIED. THIS PROCEDURECODE IS INVALID FOR THE PROVIDERPROFESSIONAL CODE (1ST DIGIT OFMODIFIER). 305 B18Payment denied/reduced becausethe payer deems the informationsubmitted does not support thislevel of service, this manyservices, this length of service,this dosage, or this day's supply.Payment denied because thisprocedure code/ modifier wasinvalid on the date of service ofclaim submission.N20M86N56Service not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.Procedure code billed is notcorrect/valid for the services billed orthe date of service billed.306307A HOSPICE RECIPIENT - RECYCLE FOR EDIT298. 106, 306 B9CLAIM/DETAIL DENIED. THIS PROCEDURECODE IS NOT PAYABLE UNLESS BILLED INCONJUNCTION WITH OTHER DESIGNATEDPROCEDURES. 307 107Services not covered because thepatient is enrolled in a Hospice. N30 Recipient ineligible for this service.Claim/service denied because therelated or qualifying claim/serviceProcedure code billed is notwas not previously paid orcorrect/valid for the services billed oridentified on this claim.N56 the date of service billed.308310311DETAIL DENIED. REQUIREDDOCUMENTATION IS MISSING OR DOES NOTVERIFY THAT MEDICAL ASSISTANCE WASPROVIDED. 180 16NEW ADMISSION NOT PAYABLE BECAUSEClaim/service lacks informationwhich is needed for adjudication.Additional information is suppliedusing remittance advice remarkscodes whenever appropriate.OF NON-COMPLIANCE 310 96 Non-covered charge(s). MA41CORRECTED PAYMENT PER ADJUSTMENTREQUEST. 125M29Missing/in<strong>com</strong>plete/invalid operativereport.Missing/in<strong>com</strong>plete/invalidaddmission type.Payment adjusted due to asubmission/billing error(s).Additional information is suppliedusing the remittance adviceremarks codes wheneverappropriate. MA67 Correction to a prior claim.316319CLAIM/DETAIL PAID. CLAIMS HISTORYREFLECTS THE TOOTH NUMBERPREVIOUSLY EXTRACTED. PLEASE CHECKRECORDS AND VERIFY TOOTH NUMBER. 316, 400 18 Duplicate claim/service. N39INCORRECT PROVIDER NUMBERSUBMITTED - PAYMENT DELAYED. 319 133The disposition of thisclaim/service is pending furtherreview.M57Procedure code is not <strong>com</strong>patiblewith tooth number/letter.Missing/in<strong>com</strong>plete/invalid provideridentifier.Page 17 of 46 Date: 3/30/2005