EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
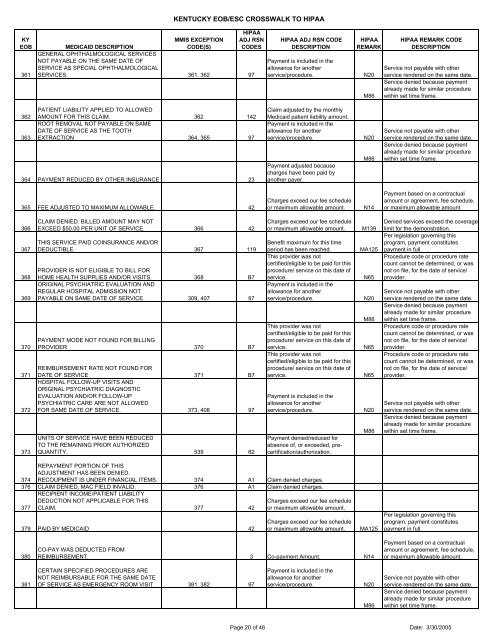
KENTUCKY <strong>EOB</strong>/ESC CROSSWALK TO HIPAAKY<strong>EOB</strong>361MMIS EXCEPTIONCODE(S)HIPAAADJ RSNCODESMEDICAID DESCRIPTIONGENERAL OPHTHALMOLOGICAL SERVICESNOT PAYABLE ON THE SAME DATE OFSERVICE AS SPECIAL OPHTHALMOLOGICALSERVICES. 361, 362 97HIPAA ADJ RSN CODEDESCRIPTIONPayment is included in theallowance for anotherservice/procedure.HIPAAREMARKN20M86HIPAA REMARK CODEDESCRIPTIONService not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.362363PATIENT LIABILITY APPLIED TO ALLOWEDAMOUNT FOR THIS CLAIM. 362 142ROOT REMOVAL NOT PAYABLE ON SAMEDATE OF SERVICE AS THE TOOTHEXTRACTION 364, 365 97364 PAYMENT REDUCED BY OTHER INSURANCE 23Claim adjusted by the monthlyMedicaid patient liability amount.Payment is included in theallowance for anotherservice/procedure.Payment adjusted becausecharges have been paid byanother payer.N20M86Service not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.365 FEE ADJUSTED TO MAXIMUM ALLOWABLE. 42Charges exceed our fee scheduleor maximum allowable amount.N14Payment based on a contractualamount or agreement, fee schedule,or maximum allowable amount.366367368369370371372373CLAIM DENIED. BILLED AMOUNT MAY NOTEXCEED $50.00 PER UNIT OF SERVICE. 366 42THIS SERVICE PAID COINSURANCE AND/ORDEDUCTIBLE. 367 119PROVIDER IS NOT ELIGIBLE TO BILL FORHOME HEALTH SUPPLIES AND/OR VISITS. 368 B7ORIGINAL PSYCHIATRIC EVALUATION ANDREGULAR HOSPITAL ADMISSION NOTPAYABLE ON SAME DATE OF SERVICE. 309, 407 97PAYMENT MODE NOT FOUND FOR BILLINGPROVIDER 370 B7REIMBURSEMENT RATE NOT FOUND FORDATE OF SERVICE 371 B7HOSPITAL FOLLOW-UP VISITS ANDORIGINAL PSYCHIATRIC DIAGNOSTICEVALUATION AND/OR FOLLOW-UPPSYCHIATRIC CARE ARE NOT ALLOWEDFOR SAME DATE OF SERVICE. 373, 408 97UNITS OF SERVICE HAVE BEEN REDUCEDTO THE REMAINING PRIOR AUTHORIZEDQUANTITY. 539 62Charges exceed our fee scheduleor maximum allowable amount.Benefit maximum for this timeperiod has been reached.This provider was notcertified/eligible to be paid for thisprocedure/ service on this date ofservice.Payment is included in theallowance for anotherservice/procedure.This provider was notcertified/eligible to be paid for thisprocedure/ service on this date ofservice.This provider was notcertified/eligible to be paid for thisprocedure/ service on this date ofservice.Payment is included in theallowance for anotherservice/procedure.Payment denied/reduced forabsence of, or exceeded, precertification/authorization.M139MA125N65N20M86N65N65N20M86Denied services exceed the coveragelimit for the demonstration.Per legislation governing thisprogram, payment constitutespayment in full.Procedure code or procedure ratecount cannot be determined, or wasnot on file, for the date of service/provider.Service not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.Procedure code or procedure ratecount cannot be determined, or wasnot on file, for the date of service/provider.Procedure code or procedure ratecount cannot be determined, or wasnot on file, for the date of service/provider.Service not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.374REPAYMENT PORTION OF THISADJUSTMENT HAS BEEN DENIED.RECOUPMENT IS UNDER FINANCIAL ITEMS. 374 A1 Claim denied charges.376 CLAIM DENIED. MAC FIELD INVALID. 376 A1 Claim denied charges.377RECIPIENT INCOME/PATIENT LIABILITYDEDUCTION NOT APPLICABLE FOR THISCLAIM. 377 42Charges exceed our fee scheduleor maximum allowable amount.379 PAID BY MEDICAID 42Charges exceed our fee scheduleor maximum allowable amount.MA125Per legislation governing thisprogram, payment constitutespayment in full.380CO-PAY WAS DEDUCTED FROMREIMBURSEMENT. 3 Co-payment Amount. N14Payment based on a contractualamount or agreement, fee schedule,or maximum allowable amount.381CERTAIN SPECIFIED PROCEDURES ARENOT REIMBURSABLE FOR THE SAME DATEOF SERVICE AS EMERGENCY ROOM VISIT 381, 382 97Payment is included in theallowance for anotherservice/procedure.N20M86Service not payable with otherservice rendered on the same date.Service denied because paymentalready made for similar procedurewithin set time frame.Page 20 of 46 Date: 3/30/2005