EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
EOB Codes and Descriptions - Kymmis.com
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
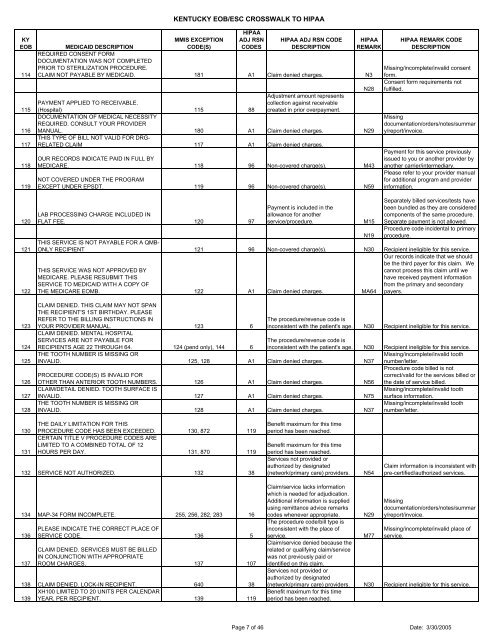
KY<strong>EOB</strong>114115116117118119KENTUCKY <strong>EOB</strong>/ESC CROSSWALK TO HIPAAMMIS EXCEPTIONCODE(S)HIPAAADJ RSNCODESHIPAA ADJ RSN CODEDESCRIPTIONHIPAAREMARKMEDICAID DESCRIPTIONREQUIRED CONSENT FORMDOCUMENTATION WAS NOT COMPLETEDPRIOR TO STERILIZATION PROCEDURE.CLAIM NOT PAYABLE BY MEDICAID. 181 A1 Claim denied charges. N3N28Adjustment amount representsPAYMENT APPLIED TO RECEIVABLE.collection against receivable(Hospital) 115 88 created in prior overpayment.DOCUMENTATION OF MEDICAL NECESSITYREQUIRED. CONSULT YOUR PROVIDERMANUAL. 180 A1 Claim denied charges. N29THIS TYPE OF BILL NOT VALID FOR DRG-RELATED CLAIM 117 A1 Claim denied charges.OUR RECORDS INDICATE PAID IN FULL BYMEDICARE. 118 96 Non-covered charge(s). M43NOT COVERED UNDER THE PROGRAMEXCEPT UNDER EPSDT. 119 96 Non-covered charge(s). N59HIPAA REMARK CODEDESCRIPTIONMissing/in<strong>com</strong>plete/invalid consentform.Consent form requirements notfulfilled.Missingdocumentation/orders/notes/summary/report/invoice.Payment for this service previouslyissued to you or another provider byanother carrier/intermediary.Please refer to your provider manualfor additional program <strong>and</strong> providerinformation.120121122123124125126127128LAB PROCESSING CHARGE INCLUDED INFLAT FEE. 120 97Payment is included in theallowance for anotherservice/procedure.M15Separately billed services/tests havebeen bundled as they are considered<strong>com</strong>ponents of the same procedure.Separate payment is not allowed.Procedure code incidental to primaryprocedure.N19THIS SERVICE IS NOT PAYABLE FOR A QMB-ONLY RECIPIENT 121 96 Non-covered charge(s). N30 Recipient ineligible for this service.Our records indicate that we shouldbe the third payer for this claim. WeTHIS SERVICE WAS NOT APPROVED BYcannot process this claim until weMEDICARE. PLEASE RESUBMIT THIShave received payment informationSERVICE TO MEDICAID WITH A COPY OFfrom the primary <strong>and</strong> secondaryTHE MEDICARE EOMB. 122 A1 Claim denied charges. MA64 payers.CLAIM DENIED. THIS CLAIM MAY NOT SPANTHE RECIPIENT'S 1ST BIRTHDAY. PLEASEREFER TO THE BILLING INSTRUCTIONS INYOUR PROVIDER MANUAL. 123 6CLAIM DENIED. MENTAL HOSPITALSERVICES ARE NOT PAYABLE FORRECIPIENTS AGE 22 THROUGH 64. 124 (pend only), 144 6The procedure/revenue code isinconsistent with the patient's age. N30 Recipient ineligible for this service.The procedure/revenue code isinconsistent with the patient's age. N30 Recipient ineligible for this service.Missing/in<strong>com</strong>plete/invalid toothnumber/letter.Procedure code billed is notcorrect/valid for the services billed orthe date of service billed.THE TOOTH NUMBER IS MISSING ORINVALID. 125, 128 A1 Claim denied charges. N37PROCEDURE CODE(S) IS INVALID FOROTHER THAN ANTERIOR TOOTH NUMBERS. 126 A1 Claim denied charges. N56CLAIM/DETAIL DENIED. TOOTH SURFACE ISINVALID. 127 A1 Claim denied charges. N75THE TOOTH NUMBER IS MISSING ORINVALID. 128 A1 Claim denied charges. N37Missing/in<strong>com</strong>plete/invalid toothsurface information.Missing/in<strong>com</strong>plete/invalid toothnumber/letter.130131THE DAILY LIMITATION FOR THISPROCEDURE CODE HAS BEEN EXCEEDED. 130, 872 119CERTAIN TITLE V PROCEDURE CODES ARELIMITED TO A COMBINED TOTAL OF 12HOURS PER DAY. 131, 870 119132 SERVICE NOT AUTHORIZED. 132 38Benefit maximum for this timeperiod has been reached.Benefit maximum for this timeperiod has been reached.Services not provided orauthorized by designated(network/primary care) providers.N54Claim information is inconsistent withpre-certified/authorized services.134 MAP-34 FORM INCOMPLETE. 255, 256, 282, 283 16136137PLEASE INDICATE THE CORRECT PLACE OFSERVICE CODE. 136 5CLAIM DENIED. SERVICES MUST BE BILLEDIN CONJUNCTION WITH APPROPRIATEROOM CHARGES. 137 107138 CLAIM DENIED. LOCK-IN RECIPIENT. 640 38XH100 LIMITED TO 20 UNITS PER CALENDAR139 YEAR, PER RECIPIENT. 139 119Claim/service lacks informationwhich is needed for adjudication.Additional information is suppliedusing remittance advice remarkscodes whenever appropriate.The procedure code/bill type isinconsistent with the place ofservice.Claim/service denied because therelated or qualifying claim/servicewas not previously paid oridentified on this claim.Services not provided orauthorized by designatedN29M77Missingdocumentation/orders/notes/summary/report/invoice.Missing/in<strong>com</strong>plete/invalid place ofservice.(network/primary care) providers. N30 Recipient ineligible for this service.Benefit maximum for this timeperiod has been reached.Page 7 of 46 Date: 3/30/2005