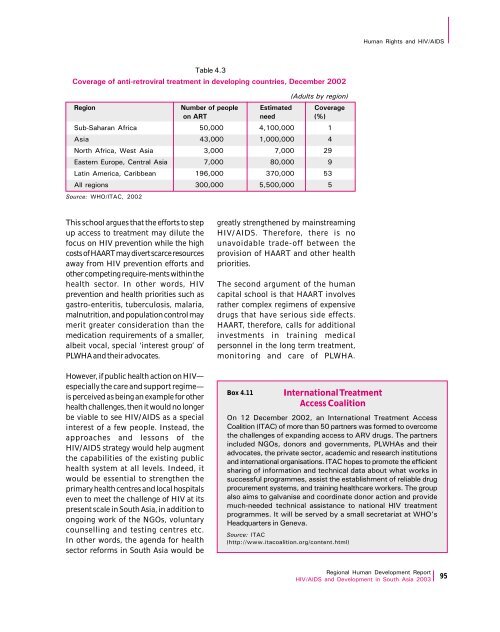
Human Rights and HIV/AIDSSource: WHO/ITAC, 2002Table 4.3Coverage of anti-retroviral treatment in developing countries, December 2002(Adults by region)Region Number of people Estimated Coverageon ART need (%)Sub-Saharan Africa 50,000 4,100,000 1<strong>Asia</strong> 43,000 1,000,000 4North Africa, West <strong>Asia</strong> 3,000 7,000 29Eastern Europe, Central <strong>Asia</strong> 7,000 80,000 9Latin America, Caribbean 196,000 370,000 53All regions 300,000 5,500,000 5This school argues that the efforts to stepup access to treatment may dilute thefocus on HIV prevention while the highcosts of HAART may divert scarce resourcesaway from HIV prevention efforts andother competing require-ments within thehealth sector. In other words, HIVprevention and health priorities such asgastro-enteritis, tuberculosis, malaria,malnutrition, and population control maymerit greater consideration than themedication requirements of a smaller,albeit vocal, special ‘interest group’ ofPLWHA and their advocates.greatly strengthened by mainstreamingHIV/AIDS. Therefore, there is nounavoidable trade-off between theprovision of HAART and other healthpriorities.The second argument of the humancapital school is that HAART involvesrather complex regimens of expensivedrugs that have serious side effects.HAART, therefore, calls for additionalinvestments in training medicalpersonnel in the long term treatment,monitoring and care of PLWHA.However, if public health action on HIV—especially the care and support regime—is perceived as being an example for otherhealth challenges, then it would no longerbe viable to see HIV/AIDS as a specialinterest of a few people. Instead, theapproaches and lessons of theHIV/AIDS strategy would help augmentthe capabilities of the existing publichealth system at all levels. Indeed, itwould be essential to strengthen theprimary health centres and local hospitalseven to meet the challenge of HIV at itspresent scale in South <strong>Asia</strong>, in addition toongoing work of the NGOs, voluntarycounselling and testing centres etc.In other words, the agenda for healthsector reforms in South <strong>Asia</strong> would beBox 4.11International TreatmentAccess CoalitionOn 12 December 2002, an International Treatment AccessCoalition (ITAC) of more than 50 partners was formed to overcomethe challenges of expanding access to ARV drugs. The partnersincluded NGOs, donors and governments, PLWHAs and theiradvocates, the private sector, academic and research institutionsand international organisations. ITAC hopes to promote the efficientsharing of information and technical data about what works insuccessful programmes, assist the establishment of reliable drugprocurement systems, and training healthcare workers. The groupalso aims to galvanise and coordinate donor action and providemuch-needed technical assistance to national HIV treatmentprogrammes. It will be served by a small secretariat at WHO’sHeadquarters in Geneva.Source: ITAC(http://www.itacoalition.org/content.html)<strong>Regional</strong> Human Development <strong>Report</strong>HIV/AIDS and Development in South <strong>Asia</strong> 2003 95
Human Rights and HIV/AIDSThe majority ofthe population,advocates of thehuman capitalschool argue, isnot literate, andgood health is notan immediatepreoccupation ofpoor households.Moreover, HAART has to be taken on afairly regular basis, life-long, implyingregular treatment expenditures for severalyears. In addition, a person living withHIV has to spend on regular medicalevaluation to monitor disease progressionas well as on treatment for themanagement of the side effects of HAART.In all the countries of South <strong>Asia</strong>, the costof HAART is significantly higher than theaverage per capita income. Access totreatment is, thus, a luxury that most South<strong>Asia</strong>n governments and the large majorityof their PLWHA cannot afford. The highcost often results in frequent interruptionof treatment, especially among the poorerpatients and this could lead to drugresistance. Presently, the private sector isthe only provider of anti-HIV treatmentsthat include ARV drugs and, in certaincases, even little understood indigenouspreparations. The haphazard provision ofARVs further underscores the urgency forgovernmental initiatives to standardiseHAART, train the health sector—bothpublic and private—and provide affordabletreatment.With South <strong>Asia</strong> bearing more than onethirdof the world’s TB burden,comprehensive national programmesbased on the free distribution of anti-TBdrugs have been in operation for severalyears. In recent times, TB controlprogrammes have also absorbed theadded cost of Directly ObservedTreatment (DOT). The TB programmesin Bangladesh, Indonesia, Nepal andMyanmar have made considerable stridesin achieving high rates of cure throughDOT, thus providing the rationale forconsidering a similar approach in the caseof HAART. Though there are few studies todemonstrate the feasibility of DOT forHAART, the approach can work amongsome groups such as sex workers orinjecting drug users.The human capital school also focuses onthe difficulties in implementing initiativesthat promote the use of HAART in aresource limited setting. The majority ofthe population, its advocates argue, is notliterate, and good health is not animmediate pre-occupation of poorhouseholds. The problem is compoundedwhen the intervention calls for complexpatterns of healthcare, in terms of thetimings and dosage of drugs, the need forancillary services such as periodic medicalreview, counselling and the managementof side-effects. The discrimination againstPLWHA even by healthcare providers andthe healthcare system in general cangreatly complicate access to HAART.This line of thinking can be countered,first, by the public obligation argument.PLWHA may be a small fraction of thetotal population in the region but, at4.2 million, their numbers are still largeand it would be a dereliction of dutynot to address the treatment, careand support of such a large number ofpeople. This argument could also bestrengthened if the morbidity and thefatality associated with HIV/AIDS is takeninto consideration. Approximately 1,000people are estimated to die every day inthe South and South East <strong>Asia</strong>n region, anumber that could be compared to twofully loaded jumbo jets crashing everyday.At 400,000 deaths in a year, the death tollfrom HIV/AIDS is nearly 400 times thecombined annual death toll from railwayaccidents. Ignoring the requirements fortreatment would involve accepting adeath toll that would be unacceptable inother contexts. Clearly, then, the ‘silentemergency’ of HIV/AIDS in South <strong>Asia</strong>requires urgent attention in ensuringaffordable and universal access totreatment, care and support.It would also be erroneous to look atprevention, care and support as mutually96<strong>Regional</strong> Human Development <strong>Report</strong>HIV/AIDS and Development in South <strong>Asia</strong> 2003