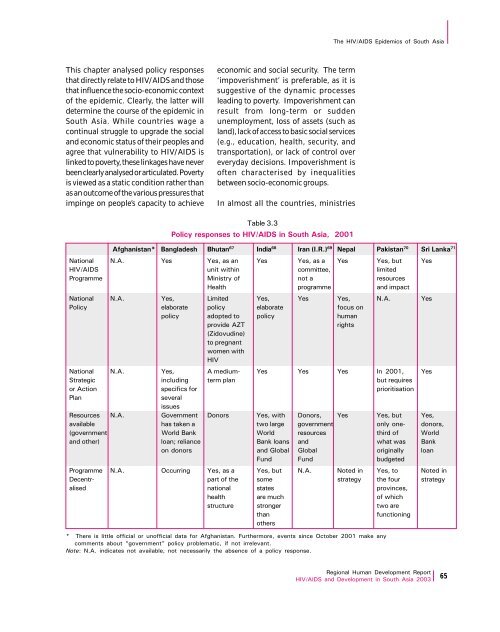
The HIV/AIDS Epidemics of South <strong>Asia</strong>This chapter analysed policy responsesthat directly relate to HIV/AIDS and thosethat influence the socio-economic contextof the epidemic. Clearly, the latter willdetermine the course of the epidemic inSouth <strong>Asia</strong>. While countries wage acontinual struggle to upgrade the socialand economic status of their peoples andagree that vulnerability to HIV/AIDS islinked to poverty, these linkages have neverbeen clearly analysed or articulated. Povertyis viewed as a static condition rather thanas an outcome of the various pressures thatimpinge on people’s capacity to achieveeconomic and social security. The term‘impoverishment’ is preferable, as it issuggestive of the dynamic processesleading to poverty. Impoverishment canresult from long-term or suddenunemployment, loss of assets (such asland), lack of access to basic social services(e.g., education, health, security, andtransportation), or lack of control overeveryday decisions. Impoverishment isoften characterised by inequalitiesbetween socio-economic groups.In almost all the countries, ministriesTable 3.3Policy responses to HIV/AIDS in South <strong>Asia</strong>, 2001Afghanistan* Bangladesh Bhutan 67 India 68 Iran (I.R.) 69 Nepal Pakistan 70 Sri Lanka 71National N.A. Yes Yes, as an Yes Yes, as a Yes Yes, but YesHIV/AIDS unit within committee, limitedProgramme Ministry of not a resourcesHealth programme and impactNational N.A. Yes, Limited Yes, Yes Yes, N.A. YesPolicy elaborate policy elaborate focus onpolicy adopted to policy humanprovide AZTrights(Zidovudine)to pregnantwomen withHIVNational N.A. Yes, A medium- Yes Yes Yes In 2001, YesStrategic including term plan but requiresor Action specifics for prioritisationPlanseveralissuesResources N.A. Government Donors Yes, with Donors, Yes Yes, but Yes,available has taken a two large government only one- donors,(government World Bank World resources third of Worldand other) loan; reliance Bank loans and what was Bankon donors and Global Global originally loanund und budgetedProgramme N.A. Occurring Yes, as a Yes, but N.A. Noted in Yes, to Noted inDecentr- part of the some strategy the four strategyalised national states provinces,health are much of whichstructure stronger two arethanfunctioningothers* There is little official or unofficial data for Afghanistan. urthermore, events since October 2001 make anycomments about “government” policy problematic, if not irrelevant.Note: N.A. indicates not available, not necessarily the absence of a policy response.<strong>Regional</strong> Human Development <strong>Report</strong>HIV/AIDS and Development in South <strong>Asia</strong> 2003 65
The HIV/AIDS Epidemics of South <strong>Asia</strong>The mechanism todeliver ‘publicgoods’ for nationalHIV/AIDSpreventionprogrammes canmove no fasterthan any other andNGOs that adopt afast track oftenfind themselves inconflict with thelaw or with theauthoritiesconcerned.other than health have seldom beeninvolved in the HIV-related policymakingprocess. Some countries haveinvolved the ministries of education andwomen’s affairs. The organisationalstructure of ministries and departmentsvaries from country to country and sodoes the relative influence wielded by oneministry vis-à-vis another. Sri Lanka, forinstance, had, at one time, a combinedMinistry of Health and Women’s Affairsand the issue of HIV and women wasapproached with a health bias. On theother hand, India and Pakistan, eachwith a separate ministry for women, wereable to bring to the problem a sharperfocus on developmental concerns ofwomen.A multi-sectoral approach has also beenslow to emerge in budgetary allocationand programme development withinministries other than health, as theseministries have been reluctant to prisefunds away from tightly controlled orlimited budgets and competing demands.Yet, countries like Bangladesh wererelatively pro-active in attempting todevelop multi-pronged programmes evenat a time when the infection rates werelow. UNAIDS estimated that at the end of2001, there were 13,000 persons withHIV/AIDS, and that 1,000 deaths due toAIDS-related infections had occurred inthat year. 72 The rates are higher in specificgroups such as injecting drug users(2.5 per cent) and commercial sex workers(0.6 per cent). 73HIV/AIDS came to be accorded highnational priority only in recent times inSouth <strong>Asia</strong>, whereas in Africa, theDeclaration on the AIDS Epidemic wasendorsed by the Heads of State andGovernment of the Organisation of AfricanUnity (OAU) in June/July 1992 itself. TheDeclaration adopted the target that: “Bythe end of 1992, each one of us will bepublicly recognised as the leader of thefight against AIDS in our country.”3.4 Challenges andImperativesSouth <strong>Asia</strong>n countries face variouschallenges in the implementation of theirnational plans of action to tackleHIV/AIDS. These challenges areheightened by the persistence of thefactors that constrain development ingeneral. The mechanism to deliver‘public goods’ for national HIV/AIDSprevention programmes can move nofaster than any other and NGOs thatadopt a fast track often find themselvesin conflict with the law or with theauthorities concerned.People living with HIV/AIDS continue tofeel isolated, neglected and deprived ofthe benefits intended for them.Urbanisation and post-liberalisationpublic culture – consumerism fuelled bygreater media exposure and a tendencytowards increased commodification ofwomen – have prompted changes in thelifestyles of the younger generation. Theseonly make them more vulnerable toinfection, underscoring the need forurgent preventive measures. Even the bestplanned programmes face formidableproblems in the South <strong>Asia</strong>n region. Thesheer magnitude of the geographical anddemographic challenges in some of thecountries, the staggering numbers ofpeople below the poverty line, low levelsof literacy, large migrant populations,inadequate health infrastructures andcompeting demands for scarce resourcesmay all conspire to relegate HIV/AIDS tothe backburner.The South <strong>Asia</strong>n Association for <strong>Regional</strong>Cooperation (SAARC) Secretariat has yetto accord HIV/AIDS priority status. South<strong>Asia</strong>n countries can benefit through66<strong>Regional</strong> Human Development <strong>Report</strong>HIV/AIDS and Development in South <strong>Asia</strong> 2003