

Swiss Medical Informatics SMI 69 - SGMI
Swiss Medical Informatics SMI 69 - SGMI
Swiss Medical Informatics SMI 69 - SGMI
WENIGER ANZEIGEN

Erfolgreiche ePaper selbst erstellen
Machen Sie aus Ihren PDF Publikationen ein blätterbares Flipbook mit unserer einzigartigen Google optimierten e-Paper Software.
PROCEEDINGS ANNUAL MEETING 2010<br />
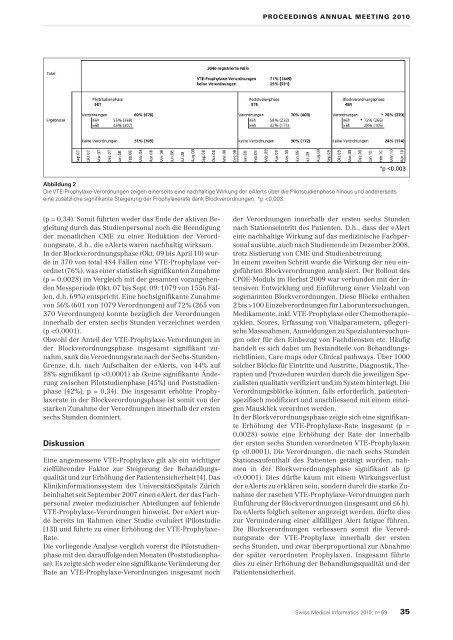
Abbildung 2<br />
Die VTE-Prophylaxe-Verordnungen zeigen einerseits eine nachhaltige Wirkung der eAlerts über die Pilotstudienphase hinaus und andererseits<br />
eine zusätzliche signifikante Steigerung der Prophylaxerate dank Blockverordnungen. *p
