

Strabismus - Fundamentals of Clinical Ophthalmology.pdf
Strabismus - Fundamentals of Clinical Ophthalmology.pdf
Strabismus - Fundamentals of Clinical Ophthalmology.pdf

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
STRABISMUS<br />
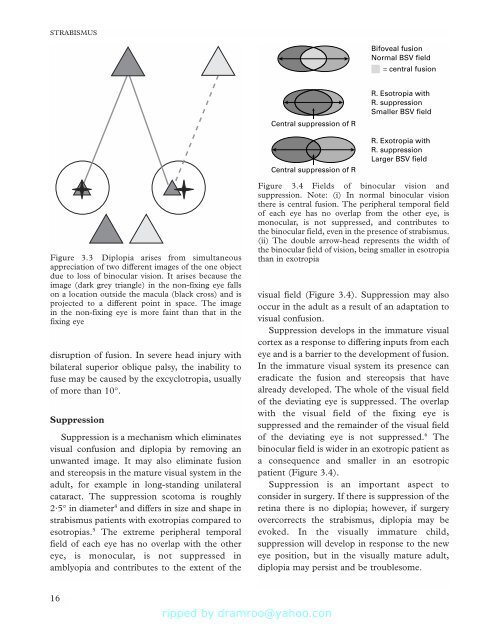
Bifoveal fusion<br />
Normal BSV field<br />
= central fusion<br />
Central suppression <strong>of</strong> R<br />
Central suppression <strong>of</strong> R<br />
R. Esotropia with<br />
R. suppression<br />
Smaller BSV field<br />
R. Exotropia with<br />
R. suppression<br />
Larger BSV field<br />
Figure 3.3 Diplopia arises from simultaneous<br />
appreciation <strong>of</strong> two different images <strong>of</strong> the one object<br />
due to loss <strong>of</strong> binocular vision. It arises because the<br />
image (dark grey triangle) in the non-fixing eye falls<br />
on a location outside the macula (black cross) and is<br />
projected to a different point in space. The image<br />
in the non-fixing eye is more faint than that in the<br />
fixing eye<br />
disruption <strong>of</strong> fusion. In severe head injury with<br />
bilateral superior oblique palsy, the inability to<br />
fuse may be caused by the excyclotropia, usually<br />
<strong>of</strong> more than 10°.<br />
Suppression<br />
Suppression is a mechanism which eliminates<br />
visual confusion and diplopia by removing an<br />
unwanted image. It may also eliminate fusion<br />
and stereopsis in the mature visual system in the<br />
adult, for example in long-standing unilateral<br />
cataract. The suppression scotoma is roughly<br />
2·5° in diameter 4 and differs in size and shape in<br />
strabismus patients with exotropias compared to<br />
esotropias. 5 The extreme peripheral temporal<br />
field <strong>of</strong> each eye has no overlap with the other<br />
eye, is monocular, is not suppressed in<br />
amblyopia and contributes to the extent <strong>of</strong> the<br />
Figure 3.4 Fields <strong>of</strong> binocular vision and<br />
suppression. Note: (i) In normal binocular vision<br />
there is central fusion. The peripheral temporal field<br />
<strong>of</strong> each eye has no overlap from the other eye, is<br />
monocular, is not suppressed, and contributes to<br />
the binocular field, even in the presence <strong>of</strong> strabismus.<br />
(ii) The double arrow-head represents the width <strong>of</strong><br />
the binocular field <strong>of</strong> vision, being smaller in esotropia<br />
than in exotropia<br />
visual field (Figure 3.4). Suppression may also<br />
occur in the adult as a result <strong>of</strong> an adaptation to<br />
visual confusion.<br />
Suppression develops in the immature visual<br />
cortex as a response to differing inputs from each<br />
eye and is a barrier to the development <strong>of</strong> fusion.<br />
In the immature visual system its presence can<br />
eradicate the fusion and stereopsis that have<br />
already developed. The whole <strong>of</strong> the visual field<br />
<strong>of</strong> the deviating eye is suppressed. The overlap<br />
with the visual field <strong>of</strong> the fixing eye is<br />
suppressed and the remainder <strong>of</strong> the visual field<br />
<strong>of</strong> the deviating eye is not suppressed. 6 The<br />
binocular field is wider in an exotropic patient as<br />
a consequence and smaller in an esotropic<br />
patient (Figure 3.4).<br />
Suppression is an important aspect to<br />
consider in surgery. If there is suppression <strong>of</strong> the<br />
retina there is no diplopia; however, if surgery<br />
overcorrects the strabismus, diplopia may be<br />
evoked. In the visually immature child,<br />
suppression will develop in response to the new<br />
eye position, but in the visually mature adult,<br />
diplopia may persist and be troublesome.<br />
16







![SISTEM SENSORY [Compatibility Mode].pdf](https://img.yumpu.com/20667975/1/190x245/sistem-sensory-compatibility-modepdf.jpg?quality=85)





