

Strabismus - Fundamentals of Clinical Ophthalmology.pdf
Strabismus - Fundamentals of Clinical Ophthalmology.pdf
Strabismus - Fundamentals of Clinical Ophthalmology.pdf

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
STRABISMUS<br />
(a)<br />
(a)<br />
(b)<br />
(b)<br />
Figure 4.17 Developmentally determined aberrant<br />
innervation resulting in the Marcus Gunn jaw winking<br />
syndrome<br />
(c)<br />
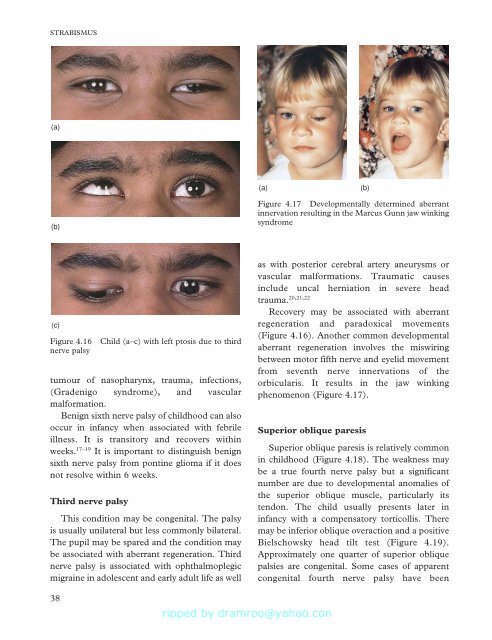
Figure 4.16<br />
nerve palsy<br />
Child (a–c) with left ptosis due to third<br />
tumour <strong>of</strong> nasopharynx, trauma, infections,<br />
(Gradenigo syndrome), and vascular<br />
malformation.<br />
Benign sixth nerve palsy <strong>of</strong> childhood can also<br />
occur in infancy when associated with febrile<br />
illness. It is transitory and recovers within<br />
weeks. 17–19 It is important to distinguish benign<br />
sixth nerve palsy from pontine glioma if it does<br />
not resolve within 6 weeks.<br />
Third nerve palsy<br />
This condition may be congenital. The palsy<br />
is usually unilateral but less commonly bilateral.<br />
The pupil may be spared and the condition may<br />
be associated with aberrant regeneration. Third<br />
nerve palsy is associated with ophthalmoplegic<br />
migraine in adolescent and early adult life as well<br />
as with posterior cerebral artery aneurysms or<br />
vascular malformations. Traumatic causes<br />
include uncal herniation in severe head<br />
trauma. 20,21,22<br />
Recovery may be associated with aberrant<br />
regeneration and paradoxical movements<br />
(Figure 4.16). Another common developmental<br />
aberrant regeneration involves the miswiring<br />
between motor fifth nerve and eyelid movement<br />
from seventh nerve innervations <strong>of</strong> the<br />
orbicularis. It results in the jaw winking<br />
phenomenon (Figure 4.17).<br />
Superior oblique paresis<br />
Superior oblique paresis is relatively common<br />
in childhood (Figure 4.18). The weakness may<br />
be a true fourth nerve palsy but a significant<br />
number are due to developmental anomalies <strong>of</strong><br />
the superior oblique muscle, particularly its<br />
tendon. The child usually presents later in<br />
infancy with a compensatory torticollis. There<br />
may be inferior oblique overaction and a positive<br />
Bielschowsky head tilt test (Figure 4.19).<br />
Approximately one quarter <strong>of</strong> superior oblique<br />
palsies are congenital. Some cases <strong>of</strong> apparent<br />
congenital fourth nerve palsy have been<br />
38







![SISTEM SENSORY [Compatibility Mode].pdf](https://img.yumpu.com/20667975/1/190x245/sistem-sensory-compatibility-modepdf.jpg?quality=85)





