National Healthcare Disparities Report - LDI Health Economist
National Healthcare Disparities Report - LDI Health Economist
National Healthcare Disparities Report - LDI Health Economist

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Care Coordination<br />
Also, in the NHQR:<br />
n Overall, rehospitalization rates did not vary by age. In some individual States, however, rates were<br />
higher among patients age 65 and over compared with patients ages 18-64.<br />
Chapter 6<br />
Medication Information<br />
Patients often seek care from many providers, and different providers may prescribe medications for the same<br />
patient. Patients are responsible for keeping track of all their medications, but medication information can be<br />
confusing, especially for patients on multiple medications. When care is not well coordinated and some providers<br />
do not know about all of a patient’s medications, patients are at greater risk for adverse events related to drug<br />
interactions, overdosing, or underdosing. In addition, providers need to periodically review all of a patient’s<br />
medications to ensure that they are taking what is needed and only what is needed. Medication reconciliation has<br />
been shown to reduce both medication errors and adverse drug events (Whittington & Cohen, 2004).<br />
Management: Provider Asking About Medications From Other Doctors<br />
Medication information generated in different settings may not be sent to a patient’s primary care provider. In<br />
the absence of communication from other providers, the patient is the primary source of medication<br />
information. Actively gathering and managing all of a patient’s medical information is an important part of<br />
care coordination.<br />
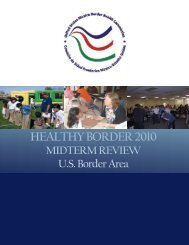
Figure 6.5. People with a usual source of care whose health provider usually asks about prescription<br />
medications and treatments from other doctors, by race and activity limitations, United States, 2002-2008<br />
100<br />
White<br />
Black<br />
Asian<br />
NHOPI<br />
AI/AN<br />
>1 Race<br />
100<br />
Basic<br />
Complex<br />
Neither Basic Nor Complex<br />
90<br />
90<br />
Percent<br />
80<br />
Percent<br />
80<br />
70<br />
70<br />
60<br />
60<br />
50<br />
Z<br />
50<br />
Z<br />
0<br />
2002<br />
2003<br />
2004<br />
2005<br />
2006<br />
2007<br />
2008<br />
0<br />
2002<br />
2003<br />
2004<br />
2005<br />
2006<br />
2007<br />
2008<br />
Key: AI/AN = American Indian or Alaska Native, NHOPI = Native Hawaiian or Other Pacific Islander.<br />
Source: Agency for <strong><strong>Health</strong>care</strong> Research and Quality, Center for Financing, Access, and Cost Trends, Medical Expenditure Panel<br />
Survey, 2002-2008.<br />
Denominator: Civilian noninstitutionalized population who report a usual source of care.<br />
Note: Data for NHOPIs were insufficient for analysis except in 2004 and 2005.<br />
186 <strong>National</strong> <strong><strong>Health</strong>care</strong> <strong>Disparities</strong> <strong>Report</strong>, 2011