

H e m a t o lo g y E d u c a t io n - European Hematology Association
H e m a t o lo g y E d u c a t io n - European Hematology Association
H e m a t o lo g y E d u c a t io n - European Hematology Association

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
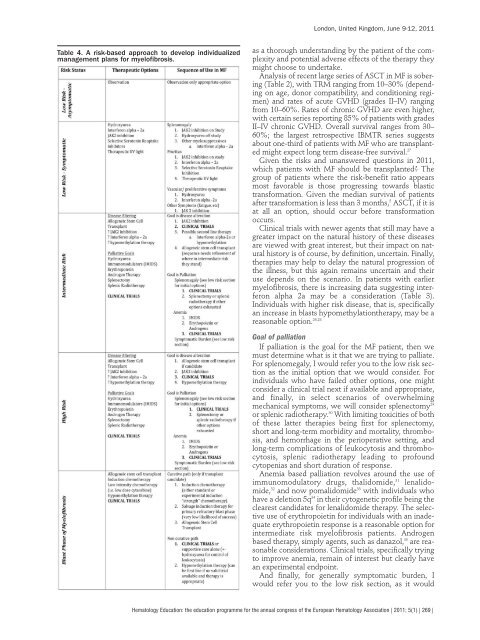
Table 4. A risk-based approach to deve<strong>lo</strong>p individualized<br />
management plans for mye<strong>lo</strong>fibrosis.<br />
London, United Kingdom, June 9-12, 2011<br />
as a thorough understanding by the patient of the complexity<br />
and potential adverse effects of the therapy they<br />
might choose to undertake.<br />
Analysis of recent large series of ASCT in MF is sobering<br />
(Table 2), with TRM ranging from 10–30% (depending<br />
on age, donor compatibility, and condit<strong>io</strong>ning regimen)<br />
and rates of acute GVHD (grades II–IV) ranging<br />
from 10–60%. Rates of chronic GVHD are even higher,<br />
with certain series reporting 85% of patients with grades<br />
II–IV chronic GVHD. Overall survival ranges from 30–<br />
60%; the largest retrospective IBMTR series suggests<br />
about one-third of patients with MF who are transplanted<br />
might expect <strong>lo</strong>ng term disease-free survival. 27<br />
Given the risks and unanswered quest<strong>io</strong>ns in 2011,<br />
which patients with MF should be transplanted? The<br />
group of patients where the risk-benefit rat<strong>io</strong> appears<br />
most favorable is those progressing towards blastic<br />
transformat<strong>io</strong>n. Given the median survival of patients<br />
after transformat<strong>io</strong>n is less than 3 months, 5 ASCT, if it is<br />
at all an opt<strong>io</strong>n, should occur before transformat<strong>io</strong>n<br />
occurs.<br />
Clinical trials with newer agents that still may have a<br />
greater impact on the natural history of these diseases<br />
are viewed with great interest, but their impact on natural<br />
history is of course, by definit<strong>io</strong>n, uncertain. Finally,<br />
therapies may help to delay the natural progress<strong>io</strong>n of<br />
the illness, but this again remains uncertain and their<br />
use depends on the scenar<strong>io</strong>. In patients with earlier<br />
mye<strong>lo</strong>fibrosis, there is increasing data suggesting interferon<br />
alpha 2a may be a considerat<strong>io</strong>n (Table 3).<br />
Individuals with higher risk disease, that is, specifically<br />
an increase in blasts hypomethylat<strong>io</strong>ntherapy, may be a<br />
reasonable opt<strong>io</strong>n. 26,28<br />
Goal of palliat<strong>io</strong>n<br />
If palliat<strong>io</strong>n is the goal for the MF patient, then we<br />
must determine what is it that we are trying to palliate.<br />
For splenomegaly, I would refer you to the <strong>lo</strong>w risk sect<strong>io</strong>n<br />
as the initial opt<strong>io</strong>n that we would consider. For<br />
individuals who have failed other opt<strong>io</strong>ns, one might<br />
consider a clinical trial next if available and appropriate,<br />
and finally, in select scenar<strong>io</strong>s of overwhelming<br />
mechanical symptoms, we will consider splenectomy 29<br />
or splenic rad<strong>io</strong>therapy. 30 With limiting toxicities of both<br />
of these latter therapies being first for splenectomy,<br />
short and <strong>lo</strong>ng-term morbidity and mortality, thrombosis,<br />
and hemorrhage in the per<strong>io</strong>perative setting, and<br />
<strong>lo</strong>ng-term complicat<strong>io</strong>ns of leukocytosis and thrombocytosis,<br />
splenic rad<strong>io</strong>therapy leading to profound<br />
cytopenias and short durat<strong>io</strong>n of response.<br />
Anemia based palliat<strong>io</strong>n revolves around the use of<br />
immunomodulatory drugs, thalidomide, 31 lenalidomide,<br />
32 and now pomalidomide 33 with individuals who<br />
have a delet<strong>io</strong>n 5q 34 in their cytogenetic profile being the<br />
clearest candidates for lenalidomide therapy. The selective<br />
use of erythropoietin for individuals with an inadequate<br />
erythropoietin response is a reasonable opt<strong>io</strong>n for<br />
intermediate risk mye<strong>lo</strong>fibrosis patients. Androgen<br />
based therapy, simply agents, such as danazol, 35 are reasonable<br />
considerat<strong>io</strong>ns. Clinical trials, specifically trying<br />
to improve anemia, remain of interest but clearly have<br />
an experimental endpoint.<br />
And finally, for generally symptomatic burden, I<br />
would refer you to the <strong>lo</strong>w risk sect<strong>io</strong>n, as it would<br />
Hemato<strong>lo</strong>gy Educat<strong>io</strong>n: the educat<strong>io</strong>n programme for the annual congress of the <strong>European</strong> Hemato<strong>lo</strong>gy Associat<strong>io</strong>n | 2011; 5(1) | 269 |









