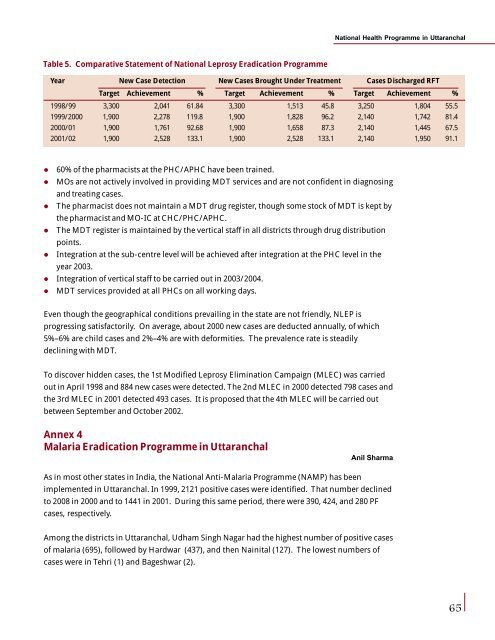
National <strong>Health</strong> Programme <strong>in</strong> UttaranchalTable 5. Comparative Statement of National Leprosy Eradication ProgrammeYear New Case Detection New Cases Brought Under Treatment Cases Discharged RFTTarget Achievement % Target Achievement % Target Achievement %1998/99 3,300 2,041 61.84 3,300 1,513 45.8 3,250 1,804 55.51999/2000 1,900 2,278 119.8 1,900 1,828 96.2 2,140 1,742 81.42000/01 1,900 1,761 92.68 1,900 1,658 87.3 2,140 1,445 67.52001/02 1,900 2,528 133.1 1,900 2,528 133.1 2,140 1,950 91.1l 60% of the pharmacists at the PHC/APHC have been tra<strong>in</strong>ed.l MOs are not actively <strong>in</strong>volved <strong>in</strong> provid<strong>in</strong>g MDT services <strong>and</strong> are not confident <strong>in</strong> diagnos<strong>in</strong>g<strong>and</strong> treat<strong>in</strong>g cases.l The pharmacist does not ma<strong>in</strong>ta<strong>in</strong> a MDT drug register, though some stock of MDT is kept bythe pharmacist <strong>and</strong> MO-IC at CHC/PHC/APHC.l The MDT register is ma<strong>in</strong>ta<strong>in</strong>ed by the vertical staff <strong>in</strong> all districts through drug distributionpo<strong>in</strong>ts.l Integration at the sub-centre level will be achieved after <strong>in</strong>tegration at the PHC level <strong>in</strong> theyear 2003.l Integration of vertical staff to be carried out <strong>in</strong> 2003/2004.l MDT services provided at all PHCs on all work<strong>in</strong>g days.Even though the geographical conditions prevail<strong>in</strong>g <strong>in</strong> the state are not friendly, NLEP isprogress<strong>in</strong>g satisfactorily. On average, about 2000 new cases are deducted annually, of which5%–6% are child cases <strong>and</strong> 2%–4% are with deformities. The prevalence rate is steadilydecl<strong>in</strong><strong>in</strong>g with MDT.To discover hidden cases, the 1st Modified Leprosy Elim<strong>in</strong>ation Campaign (MLEC) was carriedout <strong>in</strong> April 1998 <strong>and</strong> 884 new cases were detected. The 2nd MLEC <strong>in</strong> 2000 detected 798 cases <strong>and</strong>the 3rd MLEC <strong>in</strong> 2001 detected 493 cases. It is proposed that the 4th MLEC will be carried outbetween September <strong>and</strong> October 2002.Annex 4Malaria Eradication Programme <strong>in</strong> UttaranchalAnil SharmaAs <strong>in</strong> most other states <strong>in</strong> India, the National Anti-Malaria Programme (NAMP) has beenimplemented <strong>in</strong> Uttaranchal. In 1999, 2121 positive cases were identified. That number decl<strong>in</strong>edto 2008 <strong>in</strong> 2000 <strong>and</strong> to 1441 <strong>in</strong> 2001. Dur<strong>in</strong>g this same period, there were 390, 424, <strong>and</strong> 280 PFcases, respectively.Among the districts <strong>in</strong> Uttaranchal, Udham S<strong>in</strong>gh Nagar had the highest number of positive casesof malaria (695), followed by Hardwar (437), <strong>and</strong> then Na<strong>in</strong>ital (127). The lowest numbers ofcases were <strong>in</strong> Tehri (1) <strong>and</strong> Bageshwar (2).65
National <strong>Health</strong> Programme <strong>in</strong> UttaranchalTable 1. Epidemiological Situation <strong>in</strong> UttaranchalYear Population BSE Total PF Cases PF % SPR ABER API DeathsPositive Cases1999 8,138,775 686,743 2,121 390 18.38 0.31 8.43 0.26 -2000 8,316,754 148,707 2,008 424 21.10 1.35 1.78 0.24 -2001 8,479,562 128,485 1,441 280 19.40 1.12 1.52 0.16 -An exam<strong>in</strong>ation of the staff positions shows that about 66% of the DMO posts, 90% of theAssistant MO (AMO) posts, 70% of the Medical Instructor (MI)/Senior Medical Instructor (SMI)posts, 42% of the LT posts, <strong>and</strong> 44% of the Sanitary Inspector (SI)/<strong>Health</strong> Inspector (HI) postsare vacant.Capacity-build<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g for DMOs on epidemic preparedness has been conducted <strong>in</strong>Hardwar, Udham S<strong>in</strong>gh Nagar, <strong>and</strong> Dehradun. Similarily, a malariology course for PHC medicalofficers, an <strong>in</strong>troduction-level course <strong>in</strong> malaria microscopy for lab technicians, <strong>and</strong> malariatra<strong>in</strong><strong>in</strong>g for MPW/DDC/FTD have also been conducted <strong>in</strong> some districts.Through special malaria camps, 3298 blood slides were prepared, of which 28 PV positive casesgot radical treatment (RT). Also 637 general fever cases were treated at the camps.H<strong>and</strong>bills, posters, pamphlets, <strong>and</strong> wall pa<strong>in</strong>t<strong>in</strong>gs were used for IEC. In all, 129 public meet<strong>in</strong>gsfor public awareness were organized officially <strong>in</strong> Hardwar, Udham S<strong>in</strong>gh Nagar, Na<strong>in</strong>ital, <strong>and</strong>Dehradun. 178 exhibition boards received from UP were posted <strong>in</strong> all districts for impart<strong>in</strong>ghealth education <strong>and</strong> awareness about malaria.Table 2. District-wise Epidemiological Report, NAMP 2000/01District Population Total Number of P.V. Cases P.F. CasesPositive Cases2000 2001 2000 2001 2000 2001Dehradun 1,279,083 64 41 64 41 00 00Pauri 696,851 94 75 94 75 00 00Tehri 604,608 13 01 13 01 00 00Uttarkashi 294,179 06 08 06 08 00 00Chamoli 369,198 49 19 49 16 00 03Rudraprayag 227,461 00 00 00 00 00 00Hardwar 1,444,213 735 437 330 192 405 245US Nagar 1,234,548 805 695 788 663 17 32Na<strong>in</strong>ital 762,912 188 127 186 127 02 00Almora 630,446 33 15 33 15 00 00Bageshwar 249,453 00 02 00 02 00 00Pithoragarh 462,149 21 21 21 21 00 00Champawat 224,461 - - - - - -66
- Page 1 and 2:
Health Policy IssuesandHealth Progr
- Page 3 and 4:
ContentsContentsPrefaceList of Part
- Page 6 and 7:
I would also like to thank our tech
- Page 8 and 9:
List of ParticipantsIndu Kumar Pand
- Page 10 and 11:
List of ParticipantsMohmed ShaukatD
- Page 12 and 13:
List of ParticipantsR K PurohitAddi
- Page 14 and 15:
GlossaryGlossaryAbbreviationsAIIMSA
- Page 16 and 17:
GlossaryLHVLILMISMAPMCMCHMDRTBMDTM&
- Page 18 and 19:
GlossaryTHRTRCTRIPsTTTUUDCUIPUPUTVC
- Page 20 and 21:
Inaugural Sessionwould be the first
- Page 22 and 23:
Inaugural SessionOnly 18% of the pr
- Page 24 and 25:
Inaugural SessionMadhukar Gupta, Ch
- Page 26 and 27:
Inaugural Sessionrotational basis f
- Page 28 and 29:
Inaugural Sessiontell you more abou
- Page 30 and 31:
Public Health Issues, Priorities, a
- Page 32 and 33: Public Health Issues, Priorities, a
- Page 34 and 35: Public Health Issues, Priorities, a
- Page 36 and 37: Public Health Issues, Priorities, a
- Page 38 and 39: National Health Programmes: An Over
- Page 40 and 41: National Health Programmes: An Over
- Page 42 and 43: National Health Programmes: An Over
- Page 44 and 45: National Health Programmes: An Over
- Page 46 and 47: National Health Programmes: An Over
- Page 48 and 49: National Health Programmes: An Over
- Page 50 and 51: National Health Programmes: An Over
- Page 52 and 53: National Health Programmes: An Over
- Page 54 and 55: National Health Programmes: An Over
- Page 56 and 57: Implementation of National Health P
- Page 58 and 59: Implementation of National Health P
- Page 60 and 61: Implementation of National Health P
- Page 62 and 63: Implementation of National Health P
- Page 64 and 65: Implementation of National Health P
- Page 66 and 67: Use of Epidemiological Surveillance
- Page 68 and 69: Use of Epidemiological Surveillance
- Page 70 and 71: Use of Epidemiological Surveillance
- Page 72 and 73: Designing a Surveillance SystemFurt
- Page 74 and 75: Designing a Surveillance Systemsurv
- Page 76 and 77: National Health Programme in Uttara
- Page 78 and 79: National Health Programme in Uttara
- Page 80 and 81: National Health Programme in Uttara
- Page 84 and 85: National Health Programme in Uttara
- Page 86 and 87: National Health Programme in Uttara
- Page 88 and 89: National Health Programme in Uttara
- Page 90 and 91: National Health Programme in Uttara
- Page 92 and 93: National Health Programme in Uttara
- Page 94 and 95: IEC Strategies for Health in IndiaS
- Page 96 and 97: IEC Strategies for Health in Indial
- Page 98 and 99: IEC Strategies for Health in IndiaS
- Page 100 and 101: IEC Strategies for Health in IndiaA
- Page 102 and 103: IEC for Health Programmes in Uttara
- Page 104 and 105: IEC for Health Programmes in Uttara
- Page 106 and 107: IEC for Health Programmes in Uttara
- Page 108 and 109: IEC for Health Programmes in Uttara
- Page 110 and 111: IEC for Health Programmes in Uttara
- Page 112 and 113: Session 3Private and Public SectorP
- Page 114 and 115: Public-Private Interaction in Healt
- Page 116 and 117: Public-Private Interaction in Healt
- Page 118 and 119: Public-Private Interaction in Healt
- Page 120 and 121: Public-Private Interaction in Healt
- Page 122 and 123: Public-Private Interaction in Healt
- Page 124 and 125: Cost Recovery Measures in Governmen
- Page 126 and 127: Cost Recovery Measures in Governmen
- Page 128 and 129: Cost Recovery Measures in Governmen
- Page 130 and 131: Arogya Raksha: Health Insurance Sch
- Page 132 and 133:
Arogya Raksha: Health Insurance Sch
- Page 134 and 135:
Arogya Raksha: Health Insurance Sch
- Page 136 and 137:
Arogya Raksha: Health Insurance Sch
- Page 138 and 139:
Arogya Raksha: Health Insurance Sch
- Page 140 and 141:
Arogya Raksha: Health Insurance Sch
- Page 142 and 143:
Session 1Session 4Health Financing
- Page 144 and 145:
Health Financing in India: Some Iss
- Page 146 and 147:
Health Financing in India: Some Iss
- Page 148 and 149:
Health Financing in India: Some Iss
- Page 150 and 151:
Health Financing in India: Some Iss
- Page 152 and 153:
Health Financing in India: Some Iss
- Page 154 and 155:
Household Health Care Costs in Indi
- Page 156 and 157:
Household Health Care Costs in Indi
- Page 158 and 159:
Household Health Care Costs in Indi
- Page 160 and 161:
Session 1Session 4Access to Health
- Page 162 and 163:
Access to Health Services in Uttara
- Page 164 and 165:
Access to Health Services in Uttara
- Page 166 and 167:
Access to Health Services in Uttara
- Page 168 and 169:
Access to Health Services in Uttara
- Page 170 and 171:
Session 5STI/RTI, AIDS, and TB Cont
- Page 172 and 173:
Quality of RTI/STI Case Management
- Page 174 and 175:
Quality of RTI/STI Case Management
- Page 176 and 177:
Quality of RTI/STI Case Management
- Page 178 and 179:
Quality of RTI/STI Case Management
- Page 180 and 181:
Quality of RTI/STI Case Management
- Page 182 and 183:
HIV/AIDS: International Perspective
- Page 184 and 185:
HIV/AIDS: International Perspective
- Page 186 and 187:
HIV/AIDS: International Perspective
- Page 188 and 189:
HIV/AIDS in India and UttaranchalSe
- Page 190 and 191:
HIV/AIDS in India and UttaranchalFi
- Page 192 and 193:
HIV/AIDS in India and Uttaranchalpr
- Page 194 and 195:
HIV/AIDS in India and UttaranchalFi
- Page 196 and 197:
HIV/AIDS in India and UttaranchalFi
- Page 198 and 199:
Tuberculosis Control Efforts in Ind
- Page 200 and 201:
Tuberculosis Control Efforts in Ind
- Page 202 and 203:
Tuberculosis Control Efforts in Ind
- Page 204 and 205:
Tuberculosis Control Efforts in Ind
- Page 206 and 207:
Tuberculosis Control Efforts in Ind
- Page 208 and 209:
Session 6Other Health IssuesChairpe
- Page 210 and 211:
Care of the ElderlySocial care is u
- Page 212 and 213:
Care of the ElderlyEach group has d
- Page 214 and 215:
Hospital Waste ManagementSession 6H
- Page 216 and 217:
Hospital Waste ManagementA hospital
- Page 218 and 219:
Hospital Waste Managementbe without
- Page 220 and 221:
Hospital Waste ManagementTreatment
- Page 222 and 223:
Hospital Waste Management4. Tempera
- Page 224 and 225:
Hospital Waste ManagementTable 6. U
- Page 226 and 227:
Streamlining the Drug Procurement a
- Page 228 and 229:
Streamlining the Drug Procurement a
- Page 230 and 231:
Streamlining the Drug Procurement a
- Page 232 and 233:
Streamlining the Drug Procurement a
- Page 234 and 235:
Streamlining the Drug Procurement a
- Page 236 and 237:
Streamlining the Drug Procurement a
- Page 238 and 239:
Streamlining the Drug Procurement a
- Page 240 and 241:
Sanitation and Public Health Issues
- Page 242 and 243:
Sanitation and Public Health Issues
- Page 244 and 245:
Sanitation and Public Health Issues
- Page 246 and 247:
Ayurveda and Unani Department and t
- Page 248 and 249:
Ayurveda and Unani Department and t
- Page 250 and 251:
Ayurveda and Unani Department and t
- Page 252 and 253:
Specific Health Policy and Programm
- Page 254 and 255:
Specific Health Policy and Programm
- Page 256 and 257:
Specific Health Policy and Programm