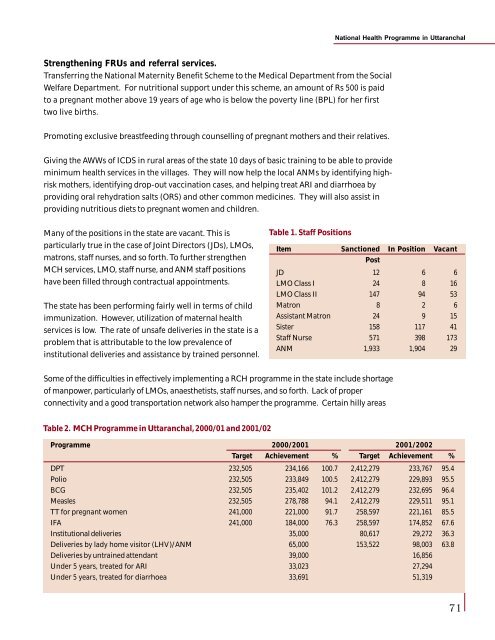
National <strong>Health</strong> Programme <strong>in</strong> UttaranchalStrengthen<strong>in</strong>g FRUs <strong>and</strong> referral services.Transferr<strong>in</strong>g the National Maternity Benefit Scheme to the Medical Department from the SocialWelfare Department. For nutritional support under this scheme, an amount of Rs 500 is paidto a pregnant mother above 19 years of age who is below the poverty l<strong>in</strong>e (BPL) for her firsttwo live births.Promot<strong>in</strong>g exclusive breastfeed<strong>in</strong>g through counsell<strong>in</strong>g of pregnant mothers <strong>and</strong> their relatives.Giv<strong>in</strong>g the AWWs of ICDS <strong>in</strong> rural areas of the state 10 days of basic tra<strong>in</strong><strong>in</strong>g to be able to providem<strong>in</strong>imum health services <strong>in</strong> the villages. They will now help the local ANMs by identify<strong>in</strong>g highriskmothers, identify<strong>in</strong>g drop-out vacc<strong>in</strong>ation cases, <strong>and</strong> help<strong>in</strong>g treat ARI <strong>and</strong> diarrhoea byprovid<strong>in</strong>g oral rehydration salts (ORS) <strong>and</strong> other common medic<strong>in</strong>es. They will also assist <strong>in</strong>provid<strong>in</strong>g nutritious diets to pregnant women <strong>and</strong> children.Many of the positions <strong>in</strong> the state are vacant. This isparticularly true <strong>in</strong> the case of Jo<strong>in</strong>t Directors (JDs), LMOs,matrons, staff nurses, <strong>and</strong> so forth. To further strengthenMCH services, LMO, staff nurse, <strong>and</strong> ANM staff positionshave been filled through contractual appo<strong>in</strong>tments.The state has been perform<strong>in</strong>g fairly well <strong>in</strong> terms of childimmunization. However, utilization of maternal healthservices is low. The rate of unsafe deliveries <strong>in</strong> the state is aproblem that is attributable to the low prevalence of<strong>in</strong>stitutional deliveries <strong>and</strong> assistance by tra<strong>in</strong>ed personnel.Table 1. Staff PositionsItem Sanctioned In Position VacantPostJD 12 6 6LMO Class I 24 8 16LMO Class II 147 94 53Matron 8 2 6Assistant Matron 24 9 15Sister 158 117 41Staff Nurse 571 398 173ANM 1,933 1,904 29Some of the difficulties <strong>in</strong> effectively implement<strong>in</strong>g a RCH programme <strong>in</strong> the state <strong>in</strong>clude shortageof manpower, particularly of LMOs, anaesthetists, staff nurses, <strong>and</strong> so forth. Lack of properconnectivity <strong>and</strong> a good transportation network also hamper the programme. Certa<strong>in</strong> hilly areasTable 2. MCH Programme <strong>in</strong> Uttaranchal, 2000/01 <strong>and</strong> 2001/02Programme 2000/2001 2001/2002Target Achievement % Target Achievement %DPT 232,505 234,166 100.7 2,412,279 233,767 95.4Polio 232,505 233,849 100.5 2,412,279 229,893 95.5BCG 232,505 235,402 101.2 2,412,279 232,695 96.4Measles 232,505 278,788 94.1 2,412,279 229,511 95.1TT for pregnant women 241,000 221,000 91.7 258,597 221,161 85.5IFA 241,000 184,000 76.3 258,597 174,852 67.6Institutional deliveries 35,000 80,617 29,272 36.3Deliveries by lady home visitor (LHV)/ANM 65,000 153,522 98,003 63.8Deliveries by untra<strong>in</strong>ed attendant 39,000 16,856Under 5 years, treated for ARI 33,023 27,294Under 5 years, treated for diarrhoea 33,691 51,31971
National <strong>Health</strong> Programme <strong>in</strong> Uttaranchalare distant <strong>and</strong> difficult to approach <strong>and</strong> the state has a poor network of roads. This is a problemparticularly dur<strong>in</strong>g w<strong>in</strong>ters <strong>and</strong> ra<strong>in</strong>y seasons. These factors lead to uncerta<strong>in</strong>ty <strong>in</strong> provid<strong>in</strong>gproper health care to pregnant mothers. Religious <strong>and</strong> social taboos also play a vital role.Suggestions for Improvementl Involvement of AWWs to tag up the health activitiesl Formation of MSS to help <strong>in</strong> the implementation of health programmesl Involvement of NGOs to organize camps, impart health education, generate healthawareness, <strong>and</strong> so forthl Involvement of gram sabha personnel <strong>in</strong> health activitiesl Empowerment of women, particularly through education, health consciousness, socialrecognition, <strong>and</strong> so forth.Annex 7HIV/AIDS Programme <strong>in</strong> UttaranchalG S JangpangiKalpana GuptaA clear-cut national health policy was formulated <strong>in</strong> 1983 <strong>and</strong> s<strong>in</strong>ce then improvements <strong>in</strong> thehealth sector have been rapidly made. As a result of the government <strong>in</strong>itiatives, several diseases,such as smallpox, have been completely eradicated <strong>and</strong> certa<strong>in</strong> other diseases, such as polio, areon the verge of be<strong>in</strong>g eradicated. Uttaranchal is a newly formed state <strong>and</strong>, like its parent state, itis attempt<strong>in</strong>g to implement the national health programmes accord<strong>in</strong>g to the guidel<strong>in</strong>es set bythe GoI.Like the dreadful plague that swept Europe dur<strong>in</strong>g the Middle Ages, HIV/AIDS is now tak<strong>in</strong>g itstoll <strong>and</strong> is pos<strong>in</strong>g a serious threat <strong>in</strong> most countries—particularly <strong>in</strong> the develop<strong>in</strong>g world. Indiais home to the largest number of people <strong>in</strong>fected with HIV <strong>in</strong> Asia. The epidemic is grow<strong>in</strong>g evenoutside the high-risk groups. Hence, this issue needs to be addressed <strong>and</strong> prevention effortsneed to be taken to ensure that HIV/AIDS rates rema<strong>in</strong> low <strong>and</strong> do not threaten development.The government needs to make efforts to erase the ignorance, mis<strong>in</strong>formation, <strong>and</strong> fear thatsurrounds the dreaded disease.The state of Uttaranchal came <strong>in</strong>to existence on 9 November 2000 <strong>and</strong> consists of 13 districts.Under the National AIDS Control Programme (NACP II), the Family <strong>Health</strong> Awareness Campaignwas launched <strong>in</strong> 1999. This campaign provides clients with RTI <strong>and</strong> STI screen<strong>in</strong>g <strong>in</strong> addition toprovid<strong>in</strong>g them with <strong>in</strong>formation on family health, misconceptions about AIDS, awareness, <strong>and</strong>so forth. The Uttaranchal State AIDS Control Society was established <strong>in</strong> April 2001 under theState Empowered Committee for National Programs of Medical <strong>Health</strong> <strong>and</strong> Family Welfare. In1996, only six districts were covered, whereas by 2000 all the districts were covered. The primeobjective of NACP II is to keep the HIV prevalence rates below one per cent, reduce blood-bornetransmission of HIV to less than one per cent, <strong>in</strong>crease the awareness level among youth <strong>and</strong>people <strong>in</strong> reproductive age groups to about 90%, <strong>and</strong> <strong>in</strong>crease the condom use among the highriskgroups, such as the commercial sex workers (CSWs), to about 90%.72
- Page 1 and 2:
Health Policy IssuesandHealth Progr
- Page 3 and 4:
ContentsContentsPrefaceList of Part
- Page 6 and 7:
I would also like to thank our tech
- Page 8 and 9:
List of ParticipantsIndu Kumar Pand
- Page 10 and 11:
List of ParticipantsMohmed ShaukatD
- Page 12 and 13:
List of ParticipantsR K PurohitAddi
- Page 14 and 15:
GlossaryGlossaryAbbreviationsAIIMSA
- Page 16 and 17:
GlossaryLHVLILMISMAPMCMCHMDRTBMDTM&
- Page 18 and 19:
GlossaryTHRTRCTRIPsTTTUUDCUIPUPUTVC
- Page 20 and 21:
Inaugural Sessionwould be the first
- Page 22 and 23:
Inaugural SessionOnly 18% of the pr
- Page 24 and 25:
Inaugural SessionMadhukar Gupta, Ch
- Page 26 and 27:
Inaugural Sessionrotational basis f
- Page 28 and 29:
Inaugural Sessiontell you more abou
- Page 30 and 31:
Public Health Issues, Priorities, a
- Page 32 and 33:
Public Health Issues, Priorities, a
- Page 34 and 35:
Public Health Issues, Priorities, a
- Page 36 and 37:
Public Health Issues, Priorities, a
- Page 38 and 39: National Health Programmes: An Over
- Page 40 and 41: National Health Programmes: An Over
- Page 42 and 43: National Health Programmes: An Over
- Page 44 and 45: National Health Programmes: An Over
- Page 46 and 47: National Health Programmes: An Over
- Page 48 and 49: National Health Programmes: An Over
- Page 50 and 51: National Health Programmes: An Over
- Page 52 and 53: National Health Programmes: An Over
- Page 54 and 55: National Health Programmes: An Over
- Page 56 and 57: Implementation of National Health P
- Page 58 and 59: Implementation of National Health P
- Page 60 and 61: Implementation of National Health P
- Page 62 and 63: Implementation of National Health P
- Page 64 and 65: Implementation of National Health P
- Page 66 and 67: Use of Epidemiological Surveillance
- Page 68 and 69: Use of Epidemiological Surveillance
- Page 70 and 71: Use of Epidemiological Surveillance
- Page 72 and 73: Designing a Surveillance SystemFurt
- Page 74 and 75: Designing a Surveillance Systemsurv
- Page 76 and 77: National Health Programme in Uttara
- Page 78 and 79: National Health Programme in Uttara
- Page 80 and 81: National Health Programme in Uttara
- Page 82 and 83: National Health Programme in Uttara
- Page 84 and 85: National Health Programme in Uttara
- Page 86 and 87: National Health Programme in Uttara
- Page 90 and 91: National Health Programme in Uttara
- Page 92 and 93: National Health Programme in Uttara
- Page 94 and 95: IEC Strategies for Health in IndiaS
- Page 96 and 97: IEC Strategies for Health in Indial
- Page 98 and 99: IEC Strategies for Health in IndiaS
- Page 100 and 101: IEC Strategies for Health in IndiaA
- Page 102 and 103: IEC for Health Programmes in Uttara
- Page 104 and 105: IEC for Health Programmes in Uttara
- Page 106 and 107: IEC for Health Programmes in Uttara
- Page 108 and 109: IEC for Health Programmes in Uttara
- Page 110 and 111: IEC for Health Programmes in Uttara
- Page 112 and 113: Session 3Private and Public SectorP
- Page 114 and 115: Public-Private Interaction in Healt
- Page 116 and 117: Public-Private Interaction in Healt
- Page 118 and 119: Public-Private Interaction in Healt
- Page 120 and 121: Public-Private Interaction in Healt
- Page 122 and 123: Public-Private Interaction in Healt
- Page 124 and 125: Cost Recovery Measures in Governmen
- Page 126 and 127: Cost Recovery Measures in Governmen
- Page 128 and 129: Cost Recovery Measures in Governmen
- Page 130 and 131: Arogya Raksha: Health Insurance Sch
- Page 132 and 133: Arogya Raksha: Health Insurance Sch
- Page 134 and 135: Arogya Raksha: Health Insurance Sch
- Page 136 and 137: Arogya Raksha: Health Insurance Sch
- Page 138 and 139:
Arogya Raksha: Health Insurance Sch
- Page 140 and 141:
Arogya Raksha: Health Insurance Sch
- Page 142 and 143:
Session 1Session 4Health Financing
- Page 144 and 145:
Health Financing in India: Some Iss
- Page 146 and 147:
Health Financing in India: Some Iss
- Page 148 and 149:
Health Financing in India: Some Iss
- Page 150 and 151:
Health Financing in India: Some Iss
- Page 152 and 153:
Health Financing in India: Some Iss
- Page 154 and 155:
Household Health Care Costs in Indi
- Page 156 and 157:
Household Health Care Costs in Indi
- Page 158 and 159:
Household Health Care Costs in Indi
- Page 160 and 161:
Session 1Session 4Access to Health
- Page 162 and 163:
Access to Health Services in Uttara
- Page 164 and 165:
Access to Health Services in Uttara
- Page 166 and 167:
Access to Health Services in Uttara
- Page 168 and 169:
Access to Health Services in Uttara
- Page 170 and 171:
Session 5STI/RTI, AIDS, and TB Cont
- Page 172 and 173:
Quality of RTI/STI Case Management
- Page 174 and 175:
Quality of RTI/STI Case Management
- Page 176 and 177:
Quality of RTI/STI Case Management
- Page 178 and 179:
Quality of RTI/STI Case Management
- Page 180 and 181:
Quality of RTI/STI Case Management
- Page 182 and 183:
HIV/AIDS: International Perspective
- Page 184 and 185:
HIV/AIDS: International Perspective
- Page 186 and 187:
HIV/AIDS: International Perspective
- Page 188 and 189:
HIV/AIDS in India and UttaranchalSe
- Page 190 and 191:
HIV/AIDS in India and UttaranchalFi
- Page 192 and 193:
HIV/AIDS in India and Uttaranchalpr
- Page 194 and 195:
HIV/AIDS in India and UttaranchalFi
- Page 196 and 197:
HIV/AIDS in India and UttaranchalFi
- Page 198 and 199:
Tuberculosis Control Efforts in Ind
- Page 200 and 201:
Tuberculosis Control Efforts in Ind
- Page 202 and 203:
Tuberculosis Control Efforts in Ind
- Page 204 and 205:
Tuberculosis Control Efforts in Ind
- Page 206 and 207:
Tuberculosis Control Efforts in Ind
- Page 208 and 209:
Session 6Other Health IssuesChairpe
- Page 210 and 211:
Care of the ElderlySocial care is u
- Page 212 and 213:
Care of the ElderlyEach group has d
- Page 214 and 215:
Hospital Waste ManagementSession 6H
- Page 216 and 217:
Hospital Waste ManagementA hospital
- Page 218 and 219:
Hospital Waste Managementbe without
- Page 220 and 221:
Hospital Waste ManagementTreatment
- Page 222 and 223:
Hospital Waste Management4. Tempera
- Page 224 and 225:
Hospital Waste ManagementTable 6. U
- Page 226 and 227:
Streamlining the Drug Procurement a
- Page 228 and 229:
Streamlining the Drug Procurement a
- Page 230 and 231:
Streamlining the Drug Procurement a
- Page 232 and 233:
Streamlining the Drug Procurement a
- Page 234 and 235:
Streamlining the Drug Procurement a
- Page 236 and 237:
Streamlining the Drug Procurement a
- Page 238 and 239:
Streamlining the Drug Procurement a
- Page 240 and 241:
Sanitation and Public Health Issues
- Page 242 and 243:
Sanitation and Public Health Issues
- Page 244 and 245:
Sanitation and Public Health Issues
- Page 246 and 247:
Ayurveda and Unani Department and t
- Page 248 and 249:
Ayurveda and Unani Department and t
- Page 250 and 251:
Ayurveda and Unani Department and t
- Page 252 and 253:
Specific Health Policy and Programm
- Page 254 and 255:
Specific Health Policy and Programm
- Page 256 and 257:
Specific Health Policy and Programm