National <strong>Health</strong> Programme <strong>in</strong> UttaranchalThere are two zonal HIV test<strong>in</strong>g centres, 10 district HIVtest<strong>in</strong>g centres, two VCTC, <strong>and</strong> 15 licensed blood banks <strong>in</strong>the state. Of the 15 licensed blood banks, 10 are managedby the government, <strong>and</strong> rema<strong>in</strong><strong>in</strong>g five by the privatesector. The state also has 9 STD cl<strong>in</strong>ics <strong>and</strong> one privatemedical college that provide facilities for HIV test<strong>in</strong>g <strong>and</strong>detection.In Uttaranchal, sent<strong>in</strong>el surveillance is conducted everyyear. This <strong>in</strong>cludes four STD cl<strong>in</strong>ics <strong>in</strong> Uttarkashi, TehriGarhwal, Dehradun, <strong>and</strong> Almora <strong>and</strong> two ANC cl<strong>in</strong>ics <strong>in</strong>Pithoragarh <strong>and</strong> Na<strong>in</strong>ital. A total of 1594 samples weretested, of which four (two male <strong>and</strong> two female patients)were found to be HIV-positive.Of the total 28,217 blood donors screened for HIV between1997 <strong>and</strong> 2001, 31 (0.1%) were reported to be HIV-positive.In 2001, a total of seven cases (two female <strong>and</strong> five malepatients) were detected as HIV-positive.Between 1998 <strong>and</strong> 2001, a total of 60 cases were found to beHIV-positive <strong>and</strong> a total of six AIDS cases were reported—one each <strong>in</strong> 1993, 1996, <strong>and</strong> 1998 <strong>and</strong> three <strong>in</strong> 1995.The total estimated targeted population was smaller <strong>in</strong>March 2002 compared with that of May 2001. About 9% ofTable 4. Total HIV-Positive Cases, 2001Table 1. Units that Exist <strong>in</strong> the State for HIV Test<strong>in</strong>g<strong>and</strong> Detection of RTI/STIZonal HIV Test<strong>in</strong>g Centre 2District HIV Test<strong>in</strong>g Centre 10Voluntary Counsell<strong>in</strong>g <strong>and</strong> Test<strong>in</strong>gCentres (VCTCs) 2Licensed Blood Bank 15(Government: 10,Private: 5)STD Cl<strong>in</strong>ics 9Medical College (Private) 1Table 2. Reports of Sent<strong>in</strong>el Surveillance(August to October 2001)Number of sent<strong>in</strong>el sites (STD Cl<strong>in</strong>ics) 4Number of sent<strong>in</strong>el sites (ANC Cl<strong>in</strong>ics) 2Number of samples tested 1594Number of samples found positive 4(Males: 2,Females: 2)Table 3. Blood Samples Screen<strong>in</strong>g Report, 1997–2001Year Number of Number HIV PercentageDonors Screened Positive1997 2,327 5 0.211998 4,001 6 0.141999 5,555 8 0.142000 5,858 9 0.152001 10,476 3 0.03Place Type of Programme HIV-Positive CasesMale Female TotalDehradun Sent<strong>in</strong>el surveillance 1 1 2Narendra NagarTehri Garhwal Sent<strong>in</strong>el surveillance 1 1 2M.H. Roorkee Blood screen<strong>in</strong>g 2 0 2H.I.H.T. Jolly Grant Dehradun Blood screen<strong>in</strong>g 1 0 1Total 5 2 7Table 5. Total HIV-Positive <strong>and</strong> AIDS Cases, 1998–2001HIV-Positive Cases AIDS CasesYear Number Year Number1998 22 1993 11999 22 1995 32000 9 1996 12001 7 1998 173
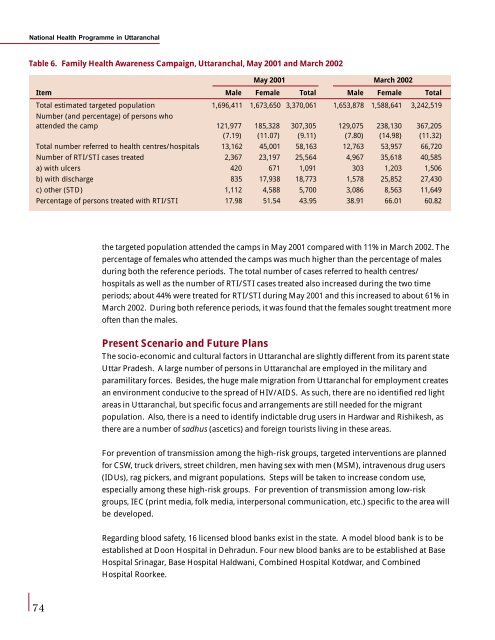
National <strong>Health</strong> Programme <strong>in</strong> UttaranchalTable 6. Family <strong>Health</strong> Awareness Campaign, Uttaranchal, May 2001 <strong>and</strong> March 2002May 2001 March 2002Item Male Female Total Male Female TotalTotal estimated targeted population 1,696,411 1,673,650 3,370,061 1,653,878 1,588,641 3,242,519Number (<strong>and</strong> percentage) of persons whoattended the camp 121,977 185,328 307,305 129,075 238,130 367,205(7.19) (11.07) (9.11) (7.80) (14.98) (11.32)Total number referred to health centres/hospitals 13,162 45,001 58,163 12,763 53,957 66,720Number of RTI/STI cases treated 2,367 23,197 25,564 4,967 35,618 40,585a) with ulcers 420 671 1,091 303 1,203 1,506b) with discharge 835 17,938 18,773 1,578 25,852 27,430c) other (STD) 1,112 4,588 5,700 3,086 8,563 11,649Percentage of persons treated with RTI/STI 17.98 51.54 43.95 38.91 66.01 60.82the targeted population attended the camps <strong>in</strong> May 2001 compared with 11% <strong>in</strong> March 2002. Thepercentage of females who attended the camps was much higher than the percentage of malesdur<strong>in</strong>g both the reference periods. The total number of cases referred to health centres/hospitals as well as the number of RTI/STI cases treated also <strong>in</strong>creased dur<strong>in</strong>g the two timeperiods; about 44% were treated for RTI/STI dur<strong>in</strong>g May 2001 <strong>and</strong> this <strong>in</strong>creased to about 61% <strong>in</strong>March 2002. Dur<strong>in</strong>g both reference periods, it was found that the females sought treatment moreoften than the males.Present Scenario <strong>and</strong> Future PlansThe socio-economic <strong>and</strong> cultural factors <strong>in</strong> Uttaranchal are slightly different from its parent stateUttar Pradesh. A large number of persons <strong>in</strong> Uttaranchal are employed <strong>in</strong> the military <strong>and</strong>paramilitary forces. Besides, the huge male migration from Uttaranchal for employment createsan environment conducive to the spread of HIV/AIDS. As such, there are no identified red lightareas <strong>in</strong> Uttaranchal, but specific focus <strong>and</strong> arrangements are still needed for the migrantpopulation. Also, there is a need to identify <strong>in</strong>dictable drug users <strong>in</strong> Hardwar <strong>and</strong> Rishikesh, asthere are a number of sadhus (ascetics) <strong>and</strong> foreign tourists liv<strong>in</strong>g <strong>in</strong> these areas.For prevention of transmission among the high-risk groups, targeted <strong>in</strong>terventions are plannedfor CSW, truck drivers, street children, men hav<strong>in</strong>g sex with men (MSM), <strong>in</strong>travenous drug users(IDUs), rag pickers, <strong>and</strong> migrant populations. Steps will be taken to <strong>in</strong>crease condom use,especially among these high-risk groups. For prevention of transmission among low-riskgroups, IEC (pr<strong>in</strong>t media, folk media, <strong>in</strong>terpersonal communication, etc.) specific to the area willbe developed.Regard<strong>in</strong>g blood safety, 16 licensed blood banks exist <strong>in</strong> the state. A model blood bank is to beestablished at Doon Hospital <strong>in</strong> Dehradun. Four new blood banks are to be established at BaseHospital Sr<strong>in</strong>agar, Base Hospital Haldwani, Comb<strong>in</strong>ed Hospital Kotdwar, <strong>and</strong> Comb<strong>in</strong>edHospital Roorkee.74
- Page 1 and 2:
Health Policy IssuesandHealth Progr
- Page 3 and 4:
ContentsContentsPrefaceList of Part
- Page 6 and 7:
I would also like to thank our tech
- Page 8 and 9:
List of ParticipantsIndu Kumar Pand
- Page 10 and 11:
List of ParticipantsMohmed ShaukatD
- Page 12 and 13:
List of ParticipantsR K PurohitAddi
- Page 14 and 15:
GlossaryGlossaryAbbreviationsAIIMSA
- Page 16 and 17:
GlossaryLHVLILMISMAPMCMCHMDRTBMDTM&
- Page 18 and 19:
GlossaryTHRTRCTRIPsTTTUUDCUIPUPUTVC
- Page 20 and 21:
Inaugural Sessionwould be the first
- Page 22 and 23:
Inaugural SessionOnly 18% of the pr
- Page 24 and 25:
Inaugural SessionMadhukar Gupta, Ch
- Page 26 and 27:
Inaugural Sessionrotational basis f
- Page 28 and 29:
Inaugural Sessiontell you more abou
- Page 30 and 31:
Public Health Issues, Priorities, a
- Page 32 and 33:
Public Health Issues, Priorities, a
- Page 34 and 35:
Public Health Issues, Priorities, a
- Page 36 and 37:
Public Health Issues, Priorities, a
- Page 38 and 39:
National Health Programmes: An Over
- Page 40 and 41: National Health Programmes: An Over
- Page 42 and 43: National Health Programmes: An Over
- Page 44 and 45: National Health Programmes: An Over
- Page 46 and 47: National Health Programmes: An Over
- Page 48 and 49: National Health Programmes: An Over
- Page 50 and 51: National Health Programmes: An Over
- Page 52 and 53: National Health Programmes: An Over
- Page 54 and 55: National Health Programmes: An Over
- Page 56 and 57: Implementation of National Health P
- Page 58 and 59: Implementation of National Health P
- Page 60 and 61: Implementation of National Health P
- Page 62 and 63: Implementation of National Health P
- Page 64 and 65: Implementation of National Health P
- Page 66 and 67: Use of Epidemiological Surveillance
- Page 68 and 69: Use of Epidemiological Surveillance
- Page 70 and 71: Use of Epidemiological Surveillance
- Page 72 and 73: Designing a Surveillance SystemFurt
- Page 74 and 75: Designing a Surveillance Systemsurv
- Page 76 and 77: National Health Programme in Uttara
- Page 78 and 79: National Health Programme in Uttara
- Page 80 and 81: National Health Programme in Uttara
- Page 82 and 83: National Health Programme in Uttara
- Page 84 and 85: National Health Programme in Uttara
- Page 86 and 87: National Health Programme in Uttara
- Page 88 and 89: National Health Programme in Uttara
- Page 92 and 93: National Health Programme in Uttara
- Page 94 and 95: IEC Strategies for Health in IndiaS
- Page 96 and 97: IEC Strategies for Health in Indial
- Page 98 and 99: IEC Strategies for Health in IndiaS
- Page 100 and 101: IEC Strategies for Health in IndiaA
- Page 102 and 103: IEC for Health Programmes in Uttara
- Page 104 and 105: IEC for Health Programmes in Uttara
- Page 106 and 107: IEC for Health Programmes in Uttara
- Page 108 and 109: IEC for Health Programmes in Uttara
- Page 110 and 111: IEC for Health Programmes in Uttara
- Page 112 and 113: Session 3Private and Public SectorP
- Page 114 and 115: Public-Private Interaction in Healt
- Page 116 and 117: Public-Private Interaction in Healt
- Page 118 and 119: Public-Private Interaction in Healt
- Page 120 and 121: Public-Private Interaction in Healt
- Page 122 and 123: Public-Private Interaction in Healt
- Page 124 and 125: Cost Recovery Measures in Governmen
- Page 126 and 127: Cost Recovery Measures in Governmen
- Page 128 and 129: Cost Recovery Measures in Governmen
- Page 130 and 131: Arogya Raksha: Health Insurance Sch
- Page 132 and 133: Arogya Raksha: Health Insurance Sch
- Page 134 and 135: Arogya Raksha: Health Insurance Sch
- Page 136 and 137: Arogya Raksha: Health Insurance Sch
- Page 138 and 139: Arogya Raksha: Health Insurance Sch
- Page 140 and 141:
Arogya Raksha: Health Insurance Sch
- Page 142 and 143:
Session 1Session 4Health Financing
- Page 144 and 145:
Health Financing in India: Some Iss
- Page 146 and 147:
Health Financing in India: Some Iss
- Page 148 and 149:
Health Financing in India: Some Iss
- Page 150 and 151:
Health Financing in India: Some Iss
- Page 152 and 153:
Health Financing in India: Some Iss
- Page 154 and 155:
Household Health Care Costs in Indi
- Page 156 and 157:
Household Health Care Costs in Indi
- Page 158 and 159:
Household Health Care Costs in Indi
- Page 160 and 161:
Session 1Session 4Access to Health
- Page 162 and 163:
Access to Health Services in Uttara
- Page 164 and 165:
Access to Health Services in Uttara
- Page 166 and 167:
Access to Health Services in Uttara
- Page 168 and 169:
Access to Health Services in Uttara
- Page 170 and 171:
Session 5STI/RTI, AIDS, and TB Cont
- Page 172 and 173:
Quality of RTI/STI Case Management
- Page 174 and 175:
Quality of RTI/STI Case Management
- Page 176 and 177:
Quality of RTI/STI Case Management
- Page 178 and 179:
Quality of RTI/STI Case Management
- Page 180 and 181:
Quality of RTI/STI Case Management
- Page 182 and 183:
HIV/AIDS: International Perspective
- Page 184 and 185:
HIV/AIDS: International Perspective
- Page 186 and 187:
HIV/AIDS: International Perspective
- Page 188 and 189:
HIV/AIDS in India and UttaranchalSe
- Page 190 and 191:
HIV/AIDS in India and UttaranchalFi
- Page 192 and 193:
HIV/AIDS in India and Uttaranchalpr
- Page 194 and 195:
HIV/AIDS in India and UttaranchalFi
- Page 196 and 197:
HIV/AIDS in India and UttaranchalFi
- Page 198 and 199:
Tuberculosis Control Efforts in Ind
- Page 200 and 201:
Tuberculosis Control Efforts in Ind
- Page 202 and 203:
Tuberculosis Control Efforts in Ind
- Page 204 and 205:
Tuberculosis Control Efforts in Ind
- Page 206 and 207:
Tuberculosis Control Efforts in Ind
- Page 208 and 209:
Session 6Other Health IssuesChairpe
- Page 210 and 211:
Care of the ElderlySocial care is u
- Page 212 and 213:
Care of the ElderlyEach group has d
- Page 214 and 215:
Hospital Waste ManagementSession 6H
- Page 216 and 217:
Hospital Waste ManagementA hospital
- Page 218 and 219:
Hospital Waste Managementbe without
- Page 220 and 221:
Hospital Waste ManagementTreatment
- Page 222 and 223:
Hospital Waste Management4. Tempera
- Page 224 and 225:
Hospital Waste ManagementTable 6. U
- Page 226 and 227:
Streamlining the Drug Procurement a
- Page 228 and 229:
Streamlining the Drug Procurement a
- Page 230 and 231:
Streamlining the Drug Procurement a
- Page 232 and 233:
Streamlining the Drug Procurement a
- Page 234 and 235:
Streamlining the Drug Procurement a
- Page 236 and 237:
Streamlining the Drug Procurement a
- Page 238 and 239:
Streamlining the Drug Procurement a
- Page 240 and 241:
Sanitation and Public Health Issues
- Page 242 and 243:
Sanitation and Public Health Issues
- Page 244 and 245:
Sanitation and Public Health Issues
- Page 246 and 247:
Ayurveda and Unani Department and t
- Page 248 and 249:
Ayurveda and Unani Department and t
- Page 250 and 251:
Ayurveda and Unani Department and t
- Page 252 and 253:
Specific Health Policy and Programm
- Page 254 and 255:
Specific Health Policy and Programm
- Page 256 and 257:
Specific Health Policy and Programm