Global Study On Child Poverty And Disparities (PDF) - Social Policy ...
Global Study On Child Poverty And Disparities (PDF) - Social Policy ...
Global Study On Child Poverty And Disparities (PDF) - Social Policy ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Trends over time<br />
Estimates from the 1999 census indicate that<br />
infant mortality was 27 per 1,000 live births and<br />
under-five mortality was 33 per 1,000 live births<br />
(Ministry of Health, MICS Survey Report, 2008).<br />
Thus the current rates (25 and 30) represent only<br />
a slight decline in the last decade, after a much<br />
sharper decline between 1990 and 1999 (see<br />
Table 4.1). <strong>Child</strong> and infant mortality rates have<br />
not been examined by region, given the small<br />
sample size of the MICS.<br />
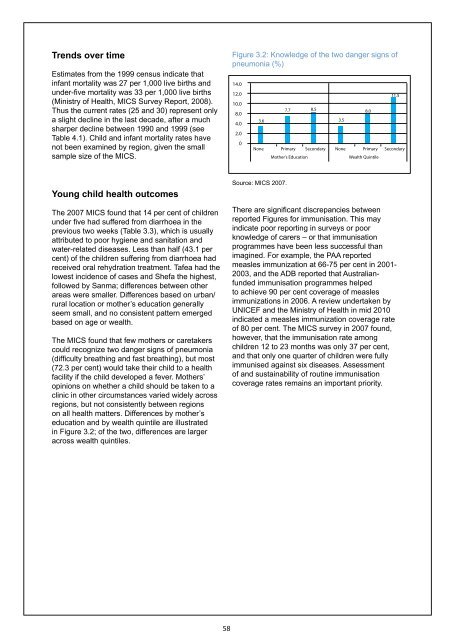
Figure 3.2: Knowledge of the two danger signs of<br />
pneumonia (%)<br />
14.0<br />
12.0<br />
10.0<br />
8.0<br />
4.0<br />
2.0<br />
0<br />
3.6<br />
7.7 8.5 8.0<br />
3.5<br />
11.5<br />
None Primary Secondary None Primary Secondary<br />
Mother’s Education<br />
Wealth Quintile<br />
Young child health outcomes<br />
The 2007 MICS found that 14 per cent of children<br />
under five had suffered from diarrhoea in the<br />
previous two weeks (Table 3.3), which is usually<br />
attributed to poor hygiene and sanitation and<br />
water-related diseases. Less than half (43.1 per<br />
cent) of the children suffering from diarrhoea had<br />
received oral rehydration treatment. Tafea had the<br />
lowest incidence of cases and Shefa the highest,<br />
followed by Sanma; differences between other<br />
areas were smaller. Differences based on urban/<br />
rural location or mother’s education generally<br />
seem small, and no consistent pattern emerged<br />
based on age or wealth.<br />
The MICS found that few mothers or caretakers<br />
could recognize two danger signs of pneumonia<br />
(difficulty breathing and fast breathing), but most<br />
(72.3 per cent) would take their child to a health<br />
facility if the child developed a fever. Mothers’<br />
opinions on whether a child should be taken to a<br />
clinic in other circumstances varied widely across<br />
regions, but not consistently between regions<br />
on all health matters. Differences by mother’s<br />
education and by wealth quintile are illustrated<br />
in Figure 3.2; of the two, differences are larger<br />
across wealth quintiles.<br />
Source: MICS 2007.<br />
There are significant discrepancies between<br />
reported Figures for immunisation. This may<br />
indicate poor reporting in surveys or poor<br />
knowledge of carers – or that immunisation<br />
programmes have been less successful than<br />
imagined. For example, the PAA reported<br />
measles immunization at 66-75 per cent in 2001-<br />
2003, and the ADB reported that Australianfunded<br />
immunisation programmes helped<br />
to achieve 90 per cent coverage of measles<br />
immunizations in 2006. A review undertaken by<br />
UNICEF and the Ministry of Health in mid 2010<br />
indicated a measles immunization coverage rate<br />
of 80 per cent. The MICS survey in 2007 found,<br />
however, that the immunisation rate among<br />
children 12 to 23 months was only 37 per cent,<br />
and that only one quarter of children were fully<br />
immunised against six diseases. Assessment<br />
of and sustainability of routine immunisation<br />
coverage rates remains an important priority.<br />
58