

Consultant physicians working with patients - Royal College of ...
Consultant physicians working with patients - Royal College of ...
Consultant physicians working with patients - Royal College of ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
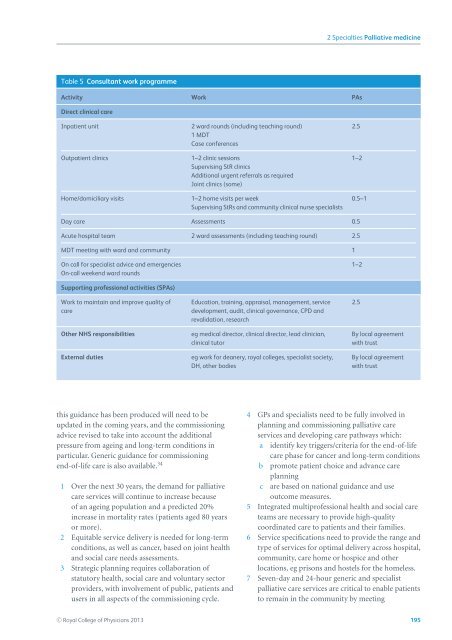
2 Specialties Palliative medicineTable 5 <strong>Consultant</strong> work programmeActivity Work PAsDirect clinical careInpatient unitOutpatient clinicsHome/domiciliary visits2 ward rounds (including teaching round)1 MDTCase conferences1–2 clinic sessionsSupervising StR clinicsAdditional urgent referrals as requiredJoint clinics (some)1–2 home visits per weekSupervising StRs and community clinical nurse specialists2.51–20.5–1Day care Assessments 0.5Acute hospital team 2 ward assessments (including teaching round) 2.5MDT meeting <strong>with</strong> ward and community 1On call for specialist advice and emergenciesOn-call weekend ward rounds1–2Supporting pr<strong>of</strong>essional activities (SPAs)Work to maintain and improve quality <strong>of</strong>careOther NHS responsibilitiesExternal dutiesEducation, training, appraisal, management, servicedevelopment, audit, clinical governance, CPD andrevalidation, researcheg medical director, clinical director, lead clinician,clinical tutoreg work for deanery, royal colleges, specialist society,DH, other bodies2.5By local agreement<strong>with</strong> trustBy local agreement<strong>with</strong> trustthis guidance has been produced will need to beupdated in the coming years, and the commissioningadvice revised to take into account the additionalpressure from ageing and long-term conditions inparticular. Generic guidance for commissioningend-<strong>of</strong>-lifecareisalsoavailable. 341 Over the next 30 years, the demand for palliativecare services will continue to increase because<strong>of</strong> an ageing population and a predicted 20%increase in mortality rates (<strong>patients</strong> aged 80 yearsor more).2 Equitable service delivery is needed for long-termconditions, as well as cancer, based on joint healthand social care needs assessments.3 Strategic planning requires collaboration <strong>of</strong>statutory health, social care and voluntary sectorproviders, <strong>with</strong> involvement <strong>of</strong> public, <strong>patients</strong> andusers in all aspects <strong>of</strong> the commissioning cycle.4 GPs and specialists need to be fully involved inplanning and commissioning palliative careservices and developing care pathways which:a identify key triggers/criteria for the end-<strong>of</strong>-lifecare phase for cancer and long-term conditionsb promote patient choice and advance careplanningc are based on national guidance and useoutcome measures.5 Integrated multipr<strong>of</strong>essional health and social careteams are necessary to provide high-qualitycoordinated care to <strong>patients</strong> and their families.6 Service specifications need to provide the range andtype <strong>of</strong> services for optimal delivery across hospital,community, care home or hospice and otherlocations, eg prisons and hostels for the homeless.7 Seven-day and 24-hour generic and specialistpalliative care services are critical to enable <strong>patients</strong>to remain in the community by meetingC○ <strong>Royal</strong> <strong>College</strong> <strong>of</strong> Physicians 2013 195














