

Consultant physicians working with patients - Royal College of ...
Consultant physicians working with patients - Royal College of ...
Consultant physicians working with patients - Royal College of ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
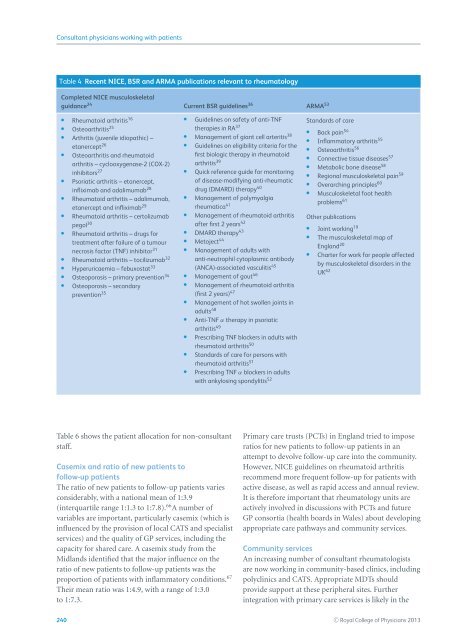
<strong>Consultant</strong> <strong>physicians</strong> <strong>working</strong> <strong>with</strong> <strong>patients</strong>Table 4 Recent NICE, BSR and ARMA publications relevant to rheumatologyCompleted NICE musculoskeletalguidance 24 Current BSR guidelines 36 ARMA 53Rheumatoid arthritis 16Osteoarthritis 25Arthritis (juvenile idiopathic) –etanercept 26Osteoarthritis and rheumatoidarthritis – cyclooxygenase-2 (COX-2)inhibitors 27Psoriatic arthritis – etanercept,infliximab and adalimumab 28Rheumatoid arthritis – adalimumab,etanercept and infliximab 29Rheumatoid arthritis – certolizumabpegol 30Rheumatoid arthritis – drugs fortreatment after failure <strong>of</strong> a tumournecrosis factor (TNF) inhibitor 31Rheumatoid arthritis – tocilizumab 32Hyperuricaemia – febuxostat 33Osteoporosis – primary prevention 34Osteoporosis – secondaryGuidelines on safety <strong>of</strong> anti-TNFtherapies in RA 37Management <strong>of</strong> giant cell arteritis38Guidelines on eligibility criteria for thefirst biologic therapy in rheumatoidarthritis39Quick reference guide for monitoring<strong>of</strong> disease-modifying anti-rheumaticdrug (DMARD) therapy40Management <strong>of</strong> polymyalgiarheumatica41Management <strong>of</strong> rheumatoid arthritisafterfirst2years 42DMARD therapy 43Metoject44Management <strong>of</strong> adults <strong>with</strong>anti-neutrophil cytoplasmic antibody(ANCA)-associated vasculitis 45Management <strong>of</strong> gout46Management <strong>of</strong> rheumatoid arthritisprevention 35 (first 2 years)47Management <strong>of</strong> hot swollen joints inadults48Anti-TNF α therapy in psoriaticarthritis49Prescribing TNF blockers in adults <strong>with</strong>rheumatoid arthritis50Standards <strong>of</strong> care for persons <strong>with</strong>rheumatoid arthritis51Prescribing TNF α blockers in adults<strong>with</strong> ankylosing spondylitis 52Standards <strong>of</strong> careBack pain 54Inflammatory arthritis 55Osteoarthritis 56Connective tissue diseases 57Metabolic bone disease 58Regional musculoskeletal pain 59Overarching principles 60Musculoskeletal foot healthproblems 61Other publicationsJoint <strong>working</strong> 19The musculoskeletal map <strong>of</strong>England 20Charter for work for people affectedby musculoskeletal disorders in theUK 62Table 6 shows the patient allocation for non-consultantstaff.Casemix and ratio <strong>of</strong> new <strong>patients</strong> t<strong>of</strong>ollow-up <strong>patients</strong>The ratio <strong>of</strong> new <strong>patients</strong> to follow-up <strong>patients</strong> variesconsiderably, <strong>with</strong> a national mean <strong>of</strong> 1:3.9(interquartile range 1:1.3 to 1:7.8). 66 Anumber<strong>of</strong>variables are important, particularly casemix (which isinfluenced by the provision <strong>of</strong> local CATS and specialistservices) and the quality <strong>of</strong> GP services, including thecapacity for shared care. A casemix study from theMidlands identified that the major influence on theratio <strong>of</strong> new <strong>patients</strong> to follow-up <strong>patients</strong> was theproportion <strong>of</strong> <strong>patients</strong> <strong>with</strong> inflammatory conditions. 67Their mean ratio was 1:4.9, <strong>with</strong> a range <strong>of</strong> 1:3.0to 1:7.3.Primary care trusts (PCTs) in England tried to imposeratios for new <strong>patients</strong> to follow-up <strong>patients</strong> in anattempt to devolve follow-up care into the community.However, NICE guidelines on rheumatoid arthritisrecommend more frequent follow-up for <strong>patients</strong> <strong>with</strong>active disease, as well as rapid access and annual review.It is therefore important that rheumatology units areactively involved in discussions <strong>with</strong> PCTs and futureGP consortia (health boards in Wales) about developingappropriate care pathways and community services.Community servicesAn increasing number <strong>of</strong> consultant rheumatologistsare now <strong>working</strong> in community-based clinics, includingpolyclinics and CATS. Appropriate MDTs shouldprovide support at these peripheral sites. Furtherintegration <strong>with</strong> primary care services is likely in the240 C○ <strong>Royal</strong> <strong>College</strong> <strong>of</strong> Physicians 2013














