used psychological theory and research to identifythe cognitive risk and protective factors that affectbehavior and then developed program activities tochange those factors, gave clear messages aboutbehavior and taught skills to avoid undesired andunprotected sexual activity. Table 1-2 lists all thedistinguishing characteristics.5. Some programs for parents also have been foundto be effective at increasing communicationbetween parents and their adolescents and atreducing adolescent sexual risk behavior(Kirby 2007).Identifying and ImprovingImportant <strong>Risk</strong> andProtective FactorsAs stated above, curriculum-based sex andSTD/HIV programs, as well as other programs,cannot directly control whether young peopleengage in sexual activity or whether they useprotection; instead, young people make their owndecisions about sexual behavior and use of protection.Thus, to be effective, programs must markedlyimprove those risk and protective factors that havean important impact on youths’ decision makingabout sexual behavior.Logically, if programs correctly identify the factorsthat have a clear impact on behavior and if programactivities markedly change those factors, then theprogram will have an impact on behavior. However,if programs identify factors that only weakly affectbehavior or fail to change the factors sufficiently,then they may not affect behavior. Consequently,it is critical both to identify the important factorsaffecting behavior and to implement programsdesigned to change those factors.Factors that have a large impact on behavior includeinternal cognitive factors (such as knowledge, attitudes,skills and intentions) and external factors suchas access to adolescent-friendly reproductive healthservices. Curriculum-based programs, especiallythose in schools, typically focus on internal cognitivefactors. These factors are very proximal (closelyTable1-1The Number of Curriculum-Based SexEducation Programs with IndicatedEffects on <strong>Sexual</strong> BehaviorsUnitedStates(N=47)OtherDevelopedCountries(N=11)DevelopingCountries(N=29)AllCountriesin the World(N=87)Initiation of Sex➤ Delayed initiation 15 2 6 23➤ Had no significant impact 17 7 16 40➤ Hastened initiation 0 0 0 0Frequency of Sex➤ Decreased frequency 6 0 4 10➤ Had no significant impact 15 1 5 21➤ Increased frequency 0 1 0 1Number of Sex Partners➤ Decreased number 11 0 5 16➤ Had no significant impact 12 0 8 20➤ Increased number 0 0 0 0Use of Condoms➤ Increased use 14 2 7 23➤ Had no significant impact 17 4 14 35➤ Decreased use 0 0 0 0Use of Contraception➤ Increased use 4 1 1 6➤ Had no significant impact 4 1 3 8➤ Decreased use 1 0 0 1<strong>Sexual</strong> <strong>Risk</strong>-Taking➤ Reduced risk 15 0 1 16➤ Had no significant impact 9 1 3 13➤ Increased risk 0 0 1 1linked to behavior conceptually) and are related tobehavior.Previous studies of curriculum-based sex and STD/HIV education programs have demonstrated thatthose programs that effectively delayed the initiationof sex, reduced the frequency of sex, or reduced thenumber of sexual partners sometimes focused onand improved the following cognitive factors (Kirby2007):1. Knowledge, including knowledge of sexual issues,pregnancy, HIV and other STDs (includingmethods of prevention)2. Perception of pregnancy risk, HIV risk, and otherSTD risk3. Personal values about sexuality and abstinence4. Perception of peer norms and behavior about sex5. Self-efficacy to refuse sexual activity and to usecondoms and contraception4 <strong>Reducing</strong> <strong>Adolescent</strong> <strong>Sexual</strong> <strong>Risk</strong>: A <strong>Theoretical</strong> Guide for Developing and Adapting Curriculum-Based Programs
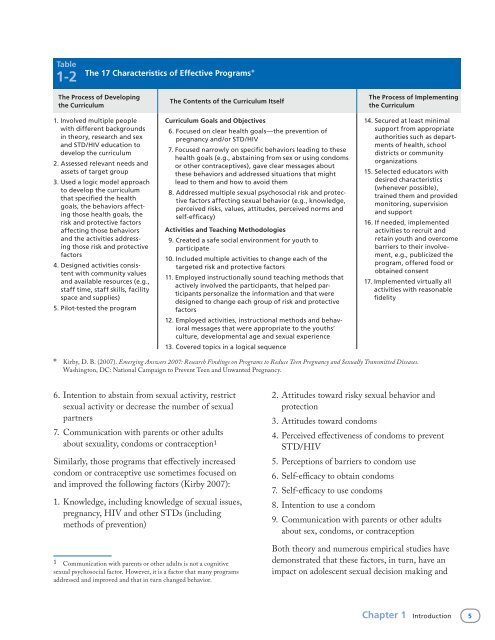
Table1-2 The 17 Characteristics of Effective Programs*The Process of Developingthe CurriculumThe Contents of the Curriculum ItselfThe Process of Implementingthe Curriculum1.Involved multiple peoplewith different backgroundsin theory, research and sexand STD/HIV education todevelop the curriculum2. Assessed relevant needs andassets of target group3. Used a logic model approachto develop the curriculumthat specified the healthgoals, the behaviors affectingthose health goals, therisk and protective factorsaffecting those behaviorsand the activities addressingthose risk and protectivefactors4. Designed activities consistentwith community valuesand available resources (e.g.,staff time, staff skills, facilityspace and supplies)5. Pilot-tested the program*Curriculum Goals and Objectives16. Focused on clear health goals—the prevention ofpregnancy and/or STD/HIV17. Focused narrowly on specific behaviors leading to thesehealth goals (e.g., abstaining from sex or using condomsor other contraceptives), gave clear messages aboutthese behaviors and addressed situations that mightlead to them and how to avoid them18. Addressed multiple sexual psychosocial risk and protectivefactors affecting sexual behavior (e.g., knowledge,perceived risks, values, attitudes, perceived norms andself-efficacy)Activities and Teaching Methodologies19. Created a safe social environment for youth toparticipate10. Included multiple activities to change each of thetargeted risk and protective factors11. Employed instructionally sound teaching methods thatactively involved the participants, that helped participantspersonalize the information and that weredesigned to change each group of risk and protectivefactors12. Employed activities, instructional methods and behavioralmessages that were appropriate to the youths’culture, developmental age and sexual experience13. Covered topics in a logical sequence14. Secured at least minimalsupport from appropriateauthorities such as departmentsof health, schooldistricts or communityorganizations15. Selected educators withdesired characteristics(whenever possible),trained them and providedmonitoring, supervisionand support16. If needed, implementedactivities to recruit andretain youth and overcomebarriers to their involvement,e.g., publicized theprogram, offered food orobtained consent17. Implemented virtually allactivities with reasonablefidelityKirby, D. B. (2007). Emerging Answers 2007: Research Findings on Programs to Reduce Teen Pregnancy and <strong>Sexual</strong>ly Transmitted Diseases.Washington, DC: National Campaign to Prevent Teen and Unwanted Pregnancy.6. Intention to abstain from sexual activity, restrictsexual activity or decrease the number of sexualpartners7. Communication with parents or other adultsabout sexuality, condoms or contraception1Similarly, those programs that effectively increasedcondom or contraceptive use sometimes focused onand improved the following factors (Kirby 2007):1. Knowledge, including knowledge of sexual issues,pregnancy, HIV and other STDs (includingmethods of prevention)1 Communication with parents or other adults is not a cognitivesexual psychosocial factor. However, it is a factor that many programsaddressed and improved and that in turn changed behavior.2. Attitudes toward risky sexual behavior andprotection3. Attitudes toward condoms4. Perceived effectiveness of condoms to preventSTD/HIV5. Perceptions of barriers to condom use6. Self-efficacy to obtain condoms7. Self-efficacy to use condoms8. Intention to use a condom9. Communication with parents or other adultsabout sex, condoms, or contraceptionBoth theory and numerous empirical studies havedemonstrated that these factors, in turn, have animpact on adolescent sexual decision making andChapter 1 Introduction 5
- Page 1: Reducing AdolescentSexual RiskA The
- Page 4 and 5: ETR Associates (Education, Training
- Page 6 and 7: AcknowledgmentsThis book evolved ou
- Page 8 and 9: Activities, Boxes and FiguresActivi
- Page 11 and 12: 1 IntroductionThis book was created
- Page 13: • Children of teenage mothers are
- Page 17: Each of the following chapters focu
- Page 20 and 21: “determinants,” “behaviors,
- Page 22 and 23: model, provide evidence regarding h
- Page 24 and 25: to avoid unwanted sex and then synt
- Page 26 and 27: Figure2-3 An Example of a Logic Mod
- Page 28 and 29: Figure2-3 An Example of a Logic Mod
- Page 30 and 31: Figure2-3 An Example of a Logic Mod
- Page 32 and 33: Table2-2Learning Objectives to Redu
- Page 34 and 35: Table2-2Learning Objectives to Redu
- Page 36 and 37: Table2-3Learning Objectives to Incr
- Page 38 and 39: Table2-4Learning Objectives to Incr
- Page 40 and 41: Table2-6Learning Objectives to Incr
- Page 43 and 44: 3 Increasing KnowledgeKeys to Incre
- Page 45 and 46: Table3-1Number of Studies Reporting
- Page 47 and 48: Box3-1Types of Activities to Increa
- Page 49 and 50: partner does not mind using a condo
- Page 51 and 52: methods more often. For example, th
- Page 53 and 54: 4ImprovingPerceptions of Risks—Bo
- Page 55 and 56: 1. Do teens’ perceptions of risk
- Page 57 and 58: a. Presentations and discussions of
- Page 59 and 60: Table4-5Examples of Items That Have
- Page 61 and 62: Pregnancy Risk Activity and Follow-
- Page 63 and 64: STD Handshake(Continued)Important C
- Page 65 and 66:
5AddressingAttitudes,Values and Bel
- Page 67 and 68:
Theories ofAttitude ChangeAttitudes
- Page 69 and 70:
Although both quality and quantity
- Page 71 and 72:
• When arguments are presented by
- Page 73 and 74:
that it is possible to improve thes
- Page 75 and 76:
c. Use simulations to demonstrate p
- Page 77 and 78:
Table5-4Examples of Survey Items fr
- Page 79 and 80:
Table5-4Examples of Survey Items fr
- Page 81 and 82:
Activity 5-2Dreams, Goals and Value
- Page 83 and 84:
Activity 5-4“Dear Abby”Descript
- Page 85 and 86:
6CorrectingPerceptionsof Peer Norms
- Page 87 and 88:
Is there a gap between perceptions
- Page 89 and 90:
3. Use concepts, language, symbols,
- Page 91 and 92:
Table6-4Examples of Items That Have
- Page 93 and 94:
7 Increasing Self-Efficacy and Skil
- Page 95 and 96:
feelings may reduce their self-effi
- Page 97 and 98:
situations more difficult so that t
- Page 99 and 100:
paper (e.g., the air should be sque
- Page 101 and 102:
Activity 7-1Lines That People Use t
- Page 103 and 104:
Situations That May Lead to Unwante
- Page 105 and 106:
Roleplaying to Enhance Refusal Skil
- Page 107:
Activity 7-5Using Condoms Correctly
- Page 110 and 111:
chaperoned, they may not have the o
- Page 112 and 113:
attitudes about condoms and contrac
- Page 114 and 115:
Activity 8-1Description of Activity
- Page 117 and 118:
9IncreasingParent-ChildCommunicatio
- Page 119 and 120:
ehavior may be quite complex (Jacca
- Page 121 and 122:
5. Give students multiple homework
- Page 123 and 124:
and the activities suggested prior
- Page 125 and 126:
Activity 9-1Description of Activity
- Page 127 and 128:
Activity 9-3Human Sexuality Board G
- Page 129 and 130:
10 ConclusionsKeys to Reducing Sexu
- Page 131 and 132:
Figure10-1Assessing Factors in Curr
- Page 133 and 134:
sexual minority youth and pressure
- Page 135 and 136:
Table10-1Instructional Principles I
- Page 137:
Table10-1Instructional Principles I
- Page 140 and 141:
Incidence The number of new cases o
- Page 143 and 144:
ResourcesThree kinds of resources a
- Page 145 and 146:
Science-Based Practices: A Guide fo
- Page 147 and 148:
National Longitudinal Study of Adol
- Page 149 and 150:
Changing Social Normshttp://www.etr
- Page 151 and 152:
Advocates for Youth, Young Women of
- Page 153 and 154:
ReferencesAbelson, R., and Prentice
- Page 155 and 156:
Coyle, K. (2006). All4You2! Prevent
- Page 157 and 158:
Lapsey, D.K. (1993). Toward an inte
- Page 159 and 160:
Weed, S.E., Olsen, J.A., DeGaston,