Although a number of possible emotional, social andhealth risks are associated with sexual intercourse,the most commonly researched risks are thoseinvolving pregnancy and STDs. This chapter, andmore generally this book, focuses on those risks.Authors use a variety of related terms involvingrisks differently or even sometimes interchangeably.For example, the following words are allcommonly used: risks, susceptibility, vulnerability,severity and seriousness. In this chapter, the “risks”associated with some course of action will refer tothe negative consequences that may result froma course of action (e.g., unintended pregnancy orSTD). “Susceptibility” will refer to the likelihood ofthose negative consequences occurring and “severity”will refer to the negative assessments of thoseconsequences.It is widely believed that some young people (perhapsa minority) feel invulnerable and that thissense of invulnerability increases their risk behavior(Weinstein 1988; Weinstein 1993; Lapsey 2003).For example, some adolescents may not think thatit is likely that they will become pregnant (or getsomeone pregnant) or that they will contract anSTD; instead, they may believe it will only happento others. According to some psychologists, adolescentsare egocentric and create “personal fables”or modes of understanding that include themes ofinvulnerability, omnipotence and personal uniqueness(Elkind 1967) and these egocentric fables arerelated to sexual risk behavior (Arnett 1990). Otherpsychologists view the creation of personal fablesand adolescents’ sense of invulnerability as adaptivemechanisms to the many challenges they face astheir egos develop (Lapsey 1993).These beliefs about invulnerability are summarizedhere because they are held by many adults workingwith youth and by some psychologists. However, astrong body of research does not yet exist to supportthese beliefs about the role of invulnerability.It is definitely true that many adolescents engagein risk behaviors because they simply do not considerthe possible risks. That is, they may engage inrisk behaviors without even assessing the possibleconsequences (Steinberg 2003). This is especiallytrue when they encounter new situations, are withtheir peers, are more oriented to the present ratherthan the future and are less able to inhibit theirimpulses (Steinberg 2003).<strong>Adolescent</strong>s’ failure to consider risks and plan effectivelymay have a biological basis. In recent years,neuroscientists have learned that adolescents’ brainscontinue to grow and change during the seconddecade of their lives. In particular, the prefrontalcortex, which affects judgment and impulse control,matures with age (Weinberger, Elvevåg et al. 2005).With a less developed prefrontal cortex, adolescentsare less likely to plan and consider risk and morelikely to be impulsive.Regardless of whether sense of invulnerability isadaptive or whether it is biologically based, manyprofessionals commonly accept that correcting adolescents’perceptions of invulnerability to pregnancyor STD has the potential to reduce their sexual riskbehavior.Perceiving risk involves recognizing the conditionsthat might lead to risk and then assessing personalrisk (Millstein 2003). The ability of teens to recognizethese situations, in turn, is affected both bytheir cognitive knowledge of the important characteristicsof the situation and by their experience withsimilar situations (Millstein 2003). Consequently,it is important for teens to review their own experiencesand those of their peers, to identify thosesituations that they or their peers encounteredthat could have led to undesired, unplanned orunprotected sex, and to describe those situationsaccurately.In sum, perceptions of risk play a central role inmany theories of health and risk behavior. Manyhealth education interventions focus on perceptionsof risk in order to improve health behaviors andreduce risk behaviors (Millstein 2003).When applying these concepts about perceptions ofrisk to sexual behavior, there are three questions thatshould be asked:44 <strong>Reducing</strong> <strong>Adolescent</strong> <strong>Sexual</strong> <strong>Risk</strong>: A <strong>Theoretical</strong> Guide for Developing and Adapting Curriculum-Based Programs
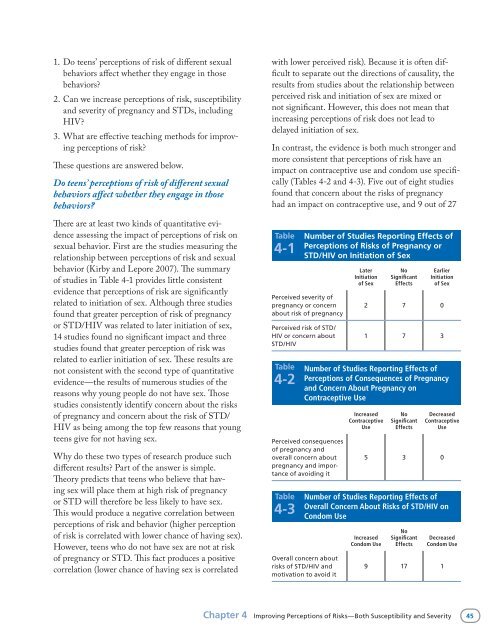
1. Do teens’ perceptions of risk of different sexualbehaviors affect whether they engage in thosebehaviors?2. Can we increase perceptions of risk, susceptibilityand severity of pregnancy and STDs, includingHIV?3. What are effective teaching methods for improvingperceptions of risk?These questions are answered below.Do teens’ perceptions of risk of different sexualbehaviors affect whether they engage in thosebehaviors?There are at least two kinds of quantitative evidenceassessing the impact of perceptions of risk onsexual behavior. First are the studies measuring therelationship between perceptions of risk and sexualbehavior (Kirby and Lepore 2007). The summaryof studies in Table 4-1 provides little consistentevidence that perceptions of risk are significantlyrelated to initiation of sex. Although three studiesfound that greater perception of risk of pregnancyor STD/HIV was related to later initiation of sex,14 studies found no significant impact and threestudies found that greater perception of risk wasrelated to earlier initiation of sex. These results arenot consistent with the second type of quantitativeevidence—the results of numerous studies of thereasons why young people do not have sex. Thosestudies consistently identify concern about the risksof pregnancy and concern about the risk of STD/HIV as being among the top few reasons that youngteens give for not having sex.Why do these two types of research produce suchdifferent results? Part of the answer is simple.Theory predicts that teens who believe that havingsex will place them at high risk of pregnancyor STD will therefore be less likely to have sex.This would produce a negative correlation betweenperceptions of risk and behavior (higher perceptionof risk is correlated with lower chance of having sex).However, teens who do not have sex are not at riskof pregnancy or STD. This fact produces a positivecorrelation (lower chance of having sex is correlatedwith lower perceived risk). Because it is often difficultto separate out the directions of causality, theresults from studies about the relationship betweenperceived risk and initiation of sex are mixed ornot significant. However, this does not mean thatincreasing perceptions of risk does not lead todelayed initiation of sex.In contrast, the evidence is both much stronger andmore consistent that perceptions of risk have animpact on contraceptive use and condom use specifically(Tables 4-2 and 4-3). Five out of eight studiesfound that concern about the risks of pregnancyhad an impact on contraceptive use, and 9 out of 27Table4-1Perceived severity ofpregnancy or concernabout risk of pregnancyPerceived risk of STD/HIV or concern aboutSTD/HIVTable4-2Number of Studies Reporting Effects ofPerceptions of <strong>Risk</strong>s of Pregnancy orSTD/HIV on Initiation of SexPerceived consequencesof pregnancy andoverall concern aboutpregnancy and importanceof avoiding itTable4-3LaterInitiationof SexNoSignificantEffectsEarlierInitiationof Sex2 7 01 7 3Number of Studies Reporting Effects ofPerceptions of Consequences of Pregnancyand Concern About Pregnancy onContraceptive UseIncreasedContraceptiveUseNoSignificantEffectsDecreasedContraceptiveUse5 3 0Number of Studies Reporting Effects ofOverall Concern About <strong>Risk</strong>s of STD/HIV onCondom UseOverall concern aboutrisks of STD/HIV andmotivation to avoid itIncreasedCondom UseNoSignificantEffectsDecreasedCondom Use9 17 1Chapter 4 Improving Perceptions of <strong>Risk</strong>s—Both Susceptibility and Severity 45
- Page 1:
Reducing AdolescentSexual RiskA The
- Page 4 and 5: ETR Associates (Education, Training
- Page 6 and 7: AcknowledgmentsThis book evolved ou
- Page 8 and 9: Activities, Boxes and FiguresActivi
- Page 11 and 12: 1 IntroductionThis book was created
- Page 13 and 14: • Children of teenage mothers are
- Page 15 and 16: Table1-2 The 17 Characteristics of
- Page 17: Each of the following chapters focu
- Page 20 and 21: “determinants,” “behaviors,
- Page 22 and 23: model, provide evidence regarding h
- Page 24 and 25: to avoid unwanted sex and then synt
- Page 26 and 27: Figure2-3 An Example of a Logic Mod
- Page 28 and 29: Figure2-3 An Example of a Logic Mod
- Page 30 and 31: Figure2-3 An Example of a Logic Mod
- Page 32 and 33: Table2-2Learning Objectives to Redu
- Page 34 and 35: Table2-2Learning Objectives to Redu
- Page 36 and 37: Table2-3Learning Objectives to Incr
- Page 38 and 39: Table2-4Learning Objectives to Incr
- Page 40 and 41: Table2-6Learning Objectives to Incr
- Page 43 and 44: 3 Increasing KnowledgeKeys to Incre
- Page 45 and 46: Table3-1Number of Studies Reporting
- Page 47 and 48: Box3-1Types of Activities to Increa
- Page 49 and 50: partner does not mind using a condo
- Page 51 and 52: methods more often. For example, th
- Page 53: 4ImprovingPerceptions of Risks—Bo
- Page 57 and 58: a. Presentations and discussions of
- Page 59 and 60: Table4-5Examples of Items That Have
- Page 61 and 62: Pregnancy Risk Activity and Follow-
- Page 63 and 64: STD Handshake(Continued)Important C
- Page 65 and 66: 5AddressingAttitudes,Values and Bel
- Page 67 and 68: Theories ofAttitude ChangeAttitudes
- Page 69 and 70: Although both quality and quantity
- Page 71 and 72: • When arguments are presented by
- Page 73 and 74: that it is possible to improve thes
- Page 75 and 76: c. Use simulations to demonstrate p
- Page 77 and 78: Table5-4Examples of Survey Items fr
- Page 79 and 80: Table5-4Examples of Survey Items fr
- Page 81 and 82: Activity 5-2Dreams, Goals and Value
- Page 83 and 84: Activity 5-4“Dear Abby”Descript
- Page 85 and 86: 6CorrectingPerceptionsof Peer Norms
- Page 87 and 88: Is there a gap between perceptions
- Page 89 and 90: 3. Use concepts, language, symbols,
- Page 91 and 92: Table6-4Examples of Items That Have
- Page 93 and 94: 7 Increasing Self-Efficacy and Skil
- Page 95 and 96: feelings may reduce their self-effi
- Page 97 and 98: situations more difficult so that t
- Page 99 and 100: paper (e.g., the air should be sque
- Page 101 and 102: Activity 7-1Lines That People Use t
- Page 103 and 104: Situations That May Lead to Unwante
- Page 105 and 106:
Roleplaying to Enhance Refusal Skil
- Page 107:
Activity 7-5Using Condoms Correctly
- Page 110 and 111:
chaperoned, they may not have the o
- Page 112 and 113:
attitudes about condoms and contrac
- Page 114 and 115:
Activity 8-1Description of Activity
- Page 117 and 118:
9IncreasingParent-ChildCommunicatio
- Page 119 and 120:
ehavior may be quite complex (Jacca
- Page 121 and 122:
5. Give students multiple homework
- Page 123 and 124:
and the activities suggested prior
- Page 125 and 126:
Activity 9-1Description of Activity
- Page 127 and 128:
Activity 9-3Human Sexuality Board G
- Page 129 and 130:
10 ConclusionsKeys to Reducing Sexu
- Page 131 and 132:
Figure10-1Assessing Factors in Curr
- Page 133 and 134:
sexual minority youth and pressure
- Page 135 and 136:
Table10-1Instructional Principles I
- Page 137:
Table10-1Instructional Principles I
- Page 140 and 141:
Incidence The number of new cases o
- Page 143 and 144:
ResourcesThree kinds of resources a
- Page 145 and 146:
Science-Based Practices: A Guide fo
- Page 147 and 148:
National Longitudinal Study of Adol
- Page 149 and 150:
Changing Social Normshttp://www.etr
- Page 151 and 152:
Advocates for Youth, Young Women of
- Page 153 and 154:
ReferencesAbelson, R., and Prentice
- Page 155 and 156:
Coyle, K. (2006). All4You2! Prevent
- Page 157 and 158:
Lapsey, D.K. (1993). Toward an inte
- Page 159 and 160:
Weed, S.E., Olsen, J.A., DeGaston,