

Anorectal Manometry in 3D NEW! - Swiss-knife.org
Anorectal Manometry in 3D NEW! - Swiss-knife.org
Anorectal Manometry in 3D NEW! - Swiss-knife.org

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
22.7<br />
Transplantation of kidneys from very young pediatric donors <strong>in</strong>to adult recipients is associated with<br />
excellent outcome<br />
T. Wolff, F. Burkhalter, T. Eugster, C. Rouden, J. Steiger, L. Gürke (Basel)<br />
Objective: The kidneys from very small donors are still often not used for transplantation <strong>in</strong>to adult<br />
recipients because of the fear of technical complications, thrombosis and poor outcome due to <strong>in</strong>sufficient<br />
renal mass.<br />
Methods: We report the retrospective analysis of all our kidney transplants <strong>in</strong>to adult recipients with<br />
kidneys from donors younger than 3 years, performed from 2004 to 2009.<br />
Results: We performed 20 transplants with donors younger than 3 years, which corresponds to 12% of<br />
the cadaveric kidney transplant performed dur<strong>in</strong>g the period of observation. Median donor age was 18<br />
months (range 5 -34 months), median donor weight was 11.5 kg (range 7.8 - 15.0 kg). Median recipient<br />
age was 49y (range 22-72y), median recipient weight was 64 kg (range 40 - 94 kg). In 18 cases<br />
the kidneys had been harvested <strong>in</strong> hospitals outside Switzerland and the <strong>org</strong>ans had been refused<br />
from all the tranplant centres <strong>in</strong> the country of orig<strong>in</strong>. In 3 recipients two kidneys were transplanted en<br />
bloc, the rema<strong>in</strong>der were s<strong>in</strong>gle kidney transplants. All kidneys were implanted <strong>in</strong> standard technique<br />
<strong>in</strong> the iliac fossa with anastomosis to the iliac vessels. In 3 cases additional surgical measures such as<br />
separate implantation of a lower pole artery or extension of a short renal ve<strong>in</strong> with saphenous ve<strong>in</strong> was<br />
required. Primary non function of the graft occurred <strong>in</strong> 2 patients (10%), once because of thrombosis<br />
of en bloc kidneys, once because of hyperacute rejection. All the rema<strong>in</strong><strong>in</strong>g grafts are function<strong>in</strong>g at<br />
present, median follow-up be<strong>in</strong>g 2y (range 0.3 - 5.9y). Median creat<strong>in</strong><strong>in</strong>e clearance one year after<br />
transplantation was 60 ml/m<strong>in</strong> (range 30 - 110). Both one year graft survival and creat<strong>in</strong><strong>in</strong>e clearance<br />
compare favorably with recipients of cadaveric adult kidneys dur<strong>in</strong>g the same period. No cases of<br />
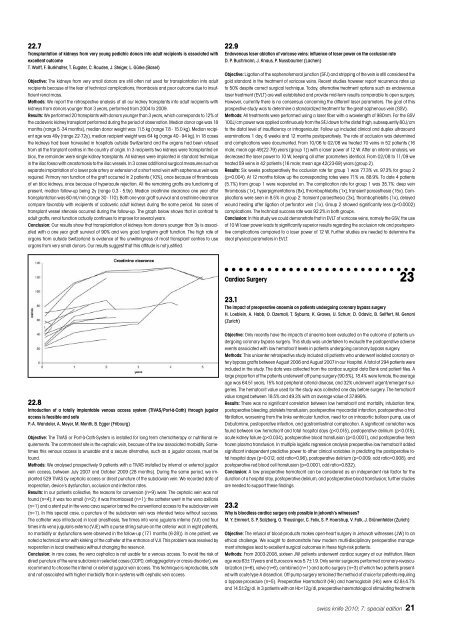
transplant vessel stenosis occurred dur<strong>in</strong>g the follow-up. The graph below shows that <strong>in</strong> contrast to<br />
adult grafts, renal function actually cont<strong>in</strong>ues to improve for several years.<br />
Conclusion: Our results show that transplantation of kidneys from donors younger than 3y is associated<br />
with a one year graft survival of 90% and very good longterm graft function. The high rate of<br />
<strong>org</strong>ans from outside Switzerland is evidence of the unwill<strong>in</strong>gness of most transplant centres to use<br />
<strong>org</strong>ans from very small donors. Our results suggest that this attitude is not justified.<br />
22.8<br />
Introduction of a totally implantable venous access system (TIVAS/Port-à-Cath) through jugular<br />
access is feasible and safe<br />
P.-A. Wandeler, A. Meyer, M. Menth, B. Egger (Fribourg)<br />
Objective: The TIVAS or Port-à-Cath-System is <strong>in</strong>stalled for long term chemotherapy or nutritional requirements.<br />
The commonest site is the cephalic ve<strong>in</strong>, because of the low associated morbidity. Sometimes<br />
this venous access is unusable and a secure alternative, such as a jugular access, must be<br />
found.<br />
Methods: We analysed prospectively 9 patients with a TIVAS <strong>in</strong>stalled by <strong>in</strong>ternal or external jugular<br />
ve<strong>in</strong> access, between July 2007 and October 2009 (28 months). Dur<strong>in</strong>g the same period, we implanted<br />
529 TIVAS by cephalic access or direct puncture of the subclavian ve<strong>in</strong>. We recorded data of<br />
reoperation, device’s dysfunction, occlusion and <strong>in</strong>fection rates.<br />
Results: In our patients collective, the reasons for conversion (n=9) were: The cephalic ve<strong>in</strong> was not<br />
found (n=4); it was too small (n=2); it was thrombosed (n=1); the catheter went <strong>in</strong> the vena axillaris<br />
(n=1) and a stent put <strong>in</strong> the vena cava superior barred the conventional access to the subclavian ve<strong>in</strong><br />
(n=1). In this special case, a puncture of the subclavian ve<strong>in</strong> was <strong>in</strong>tended twice without success.<br />
The catheter was <strong>in</strong>troduced <strong>in</strong> local anesthesia, five times <strong>in</strong>to vena jugularis <strong>in</strong>terna (VJI) and four<br />
times <strong>in</strong>to vena jugularis externa (VJE) with a purse str<strong>in</strong>g suture on the anterior wall. In eight patients,<br />
no morbidity or dysfunctions were observed <strong>in</strong> the follow-up (17.1 months [6-28]). In one patient, we<br />
noted a technical error with k<strong>in</strong>k<strong>in</strong>g of the catheter at the entrance of VJI. This problem was resolved by<br />
reoperation <strong>in</strong> local anesthesia without chang<strong>in</strong>g the reservoir.<br />
Conclusion: In rare cases, the vena cephalica is not usable for a venous access. To avoid the risk of<br />
direct puncture of the vena subclavia <strong>in</strong> selected cases (COPD, antiaggregatory or crasis disorder), we<br />
recommend to choose the <strong>in</strong>ternal or external jugular ve<strong>in</strong> access. This technique is reproducible, safe<br />
and not associated with higher morbidity than <strong>in</strong> systems with cephalic ve<strong>in</strong> access.<br />
22.9<br />
Endovenous laser ablation of varicose ve<strong>in</strong>s: <strong>in</strong>fluence of laser power on the occlusion rate<br />
D. P. Buchmann, J. Knaus, P. Nussbaumer (Lachen)<br />
Objective: Ligation of the saphenofemoral junction (SFJ) and stripp<strong>in</strong>g of the ve<strong>in</strong> is still considered the<br />
gold standard <strong>in</strong> the treatment of varicose ve<strong>in</strong>s. Recent studies however report recurrence rates up<br />
to 50% despite correct surgical technique. Today, alternative treatment options such as endovenous<br />
laser treatment (EVLT) are well established and provide mid-term results comparable to open surgery.<br />
However, currently there is no consensus concern<strong>in</strong>g the different laser parameters. The goal of this<br />
prospective study was to determ<strong>in</strong>e a standardized treatment for the great saphenous ve<strong>in</strong> (GSV).<br />
Methods: All treatments were performed us<strong>in</strong>g a laser fiber with a wavelength of 980nm. For the GSV<br />
100J/cm power was applied cont<strong>in</strong>uously from the SFJ down to the distal thigh, subsequently 80J/cm<br />
to the distal level of <strong>in</strong>sufficiency or <strong>in</strong>fragenicular. Follow up <strong>in</strong>cluded cl<strong>in</strong>ical and duplex ultrasound<br />
exam<strong>in</strong>ations 1 day, 6 weeks and 12 months postoperatively. The rate of occlusion was determ<strong>in</strong>ed<br />
and complications were documented. From 10/06 to 02/08 we treated 70 ve<strong>in</strong>s <strong>in</strong> 52 patients (16<br />
male; mean age 49(22-79) years (group 1)) with a laser power of 12 W. After an <strong>in</strong>terim analysis, we<br />
decreased the laser power to 10 W, keep<strong>in</strong>g all other parameters identical. From 02/08 to 11/09 we<br />
treated 59 ve<strong>in</strong>s <strong>in</strong> 42 patients (16 male; mean age 42(23-69) years (group 2).<br />
Results: Six weeks postoperatively the occlusion rate for group 1 was 77.3% vs. 97.3% for group 2<br />
(p=0.004). At 12 months follow up the correspond<strong>in</strong>g rates were 71% vs. 88.9%. To date 4 patients<br />
(5.7%) from group 1 were reoperated on. The complication rate for group 1 was 35.7%: deep ve<strong>in</strong><br />
thrombosis (1x), hyperpigmentations (8x), thrombophlebitis (1x), transient paraesthesia (15x). Complications<br />
were seen <strong>in</strong> 8.5% <strong>in</strong> group 2: transient paraesthesia (3x), thrombophlebitis (1x), delayed<br />
wound heal<strong>in</strong>g after ligation of perforator ve<strong>in</strong> (1x). Group 2 showed significantly less (p













