

Anorectal Manometry in 3D NEW! - Swiss-knife.org
Anorectal Manometry in 3D NEW! - Swiss-knife.org
Anorectal Manometry in 3D NEW! - Swiss-knife.org

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
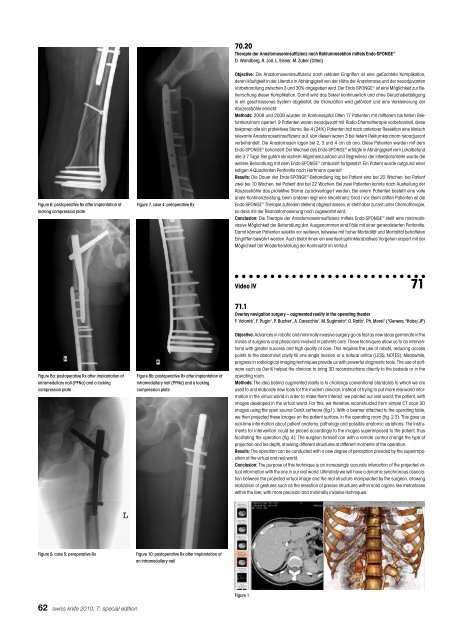
Figure 6: postoperative Rx after implantation of Figure 7, case 4: preoperative Rx<br />
lock<strong>in</strong>g compression plate<br />
Figure 8a: postoperative Rx after implantation of Figure 8b: postoperative Rx after implantation of<br />
<strong>in</strong>tramedullary nail (PFNa) and a lock<strong>in</strong>g <strong>in</strong>tramedullary nail (PFNa) and a lock<strong>in</strong>g<br />
compression plate compression plate<br />
Figure 9, case 5: peroperative Rx Figure 10: postoperative Rx after implantation of<br />
an <strong>in</strong>tramedullary nail<br />
62 swiss <strong>knife</strong> 2010; 7: special edition<br />
70.20<br />
Therapie der Anastomosen<strong>in</strong>suffizienz nach Rektumresektion mittels Endo-SPONGE ®<br />
D. Wondberg, R. Jori, L. Eisner, M. Zuber (Olten)<br />
Objective: Die Anastomosen<strong>in</strong>suffizienz nach rektalen E<strong>in</strong>griffen ist e<strong>in</strong>e gefürchtete Komplikation,<br />
deren Häufigkeit <strong>in</strong> der Literatur <strong>in</strong> Abhängigkeit von der Höhe der Anastomose und der neoadjuvanten<br />
Vorbehandlung zwischen 3 und 30% angegeben wird. Der Endo-SPONGE ® ist e<strong>in</strong>e Möglichkeit zur Beherrschung<br />
dieser Komplikation. Damit wird das Sekret kont<strong>in</strong>uierlich und ohne Geruchsbelästigung<br />
<strong>in</strong> e<strong>in</strong> geschlossenes System abgeleitet, die Granulation wird gefördert und e<strong>in</strong>e Verkle<strong>in</strong>erung der<br />
Abszesshöhle erreicht.<br />
Methods: 2008 und 2009 wurden im Kantonsspital Olten 17 Patienten mit mittlerem bis tiefem Rektumkarz<strong>in</strong>om<br />
operiert. 9 Patienten waren neoadjuvant mit Radio-Chemotherapie vorbehandelt, diese<br />
bekamen alle e<strong>in</strong> protektives Stoma. Bei 4 (24%) Patienten trat nach anteriorer Resektion e<strong>in</strong>e kl<strong>in</strong>isch<br />
relevante Anastomosen<strong>in</strong>suffizienz auf. Von diesen waren 3 bei tiefem Rektumkarz<strong>in</strong>om neoadjuvant<br />
vorbehandelt. Die Anastomosen lagen bei 2, 3 und 4 cm ab ano. Diese Patienten wurden mit dem<br />
Endo-SPONGE ® behandelt. Der Wechsel des Endo-SPONGE ® erfolgte <strong>in</strong> Abhängigkeit vom Lokalbefund<br />
alle 3-7 Tage. Bei gutem kl<strong>in</strong>ischem Allgeme<strong>in</strong>zustand und Regredienz der Infektparameter wurde die<br />
weitere Behandlung mit dem Endo-SPONGE ® ambulant fortgesetzt. E<strong>in</strong> Patient wurde aufgrund e<strong>in</strong>er<br />
kotigen 4-Quadranten Peritonitis nach Hartmann operiert.<br />
Results: Die Dauer der Endo-SPONGE ® -Behandlung lag bei Patient e<strong>in</strong>s bei 20 Wochen, bei Patient<br />
zwei bei 10 Wochen, bei Patient drei bei 22 Wochen. Bei zwei Patienten konnte nach Ausheilung der<br />
Abszesshöhle das protektive Stoma zurückverlagert werden. Bei e<strong>in</strong>em Patienten besteht e<strong>in</strong>e volle<br />
anale Kont<strong>in</strong>enzleistung, beim anderen liegt e<strong>in</strong>e Inkont<strong>in</strong>enz Grad I vor. Beim dritten Patienten ist die<br />
Endo-SPONGE ® Therapie zufrieden stellend abgeschlossen, er steht aber zurzeit unter Chemotherapie,<br />
so dass mit der Reanastomosierung noch zugewartet wird.<br />
Conclusion: Die Therapie der Anastomosen<strong>in</strong>suffizienz mittels Endo-SPONGE ® stellt e<strong>in</strong>e m<strong>in</strong>imal<strong>in</strong>vasive<br />
Möglichkeit der Behandlung dar. Ausgenommen s<strong>in</strong>d Fälle mit e<strong>in</strong>er generalisierten Peritonitis.<br />
Damit können Patienten selektiv vor weiteren, teilweise mit hoher Morbidität und Mortalität behafteten<br />
E<strong>in</strong>griffen bewahrt werden. Auch bleibt ihnen e<strong>in</strong> eventuell sph<strong>in</strong>kterablatives V<strong>org</strong>ehen erspart mit der<br />
Möglichkeit der Wiederherstellung der Kont<strong>in</strong>uität im Verlauf.<br />
Video IV 71<br />
71.1<br />
Overlay navigation surgery – augmented reality <strong>in</strong> the operat<strong>in</strong>g theater<br />
F. Volonté 1 , F. Pug<strong>in</strong> 1 , P. Bucher 1 , A. Carecchio 1 , M. Sugimoto 2 , O. Ratib 1 , Ph. Morel 1 ( 1 Geneva, 2 Kobe/JP)<br />
Objective: Advances <strong>in</strong> robotic and m<strong>in</strong>imally <strong>in</strong>vasive surgery go as fast as new ideas germ<strong>in</strong>ate <strong>in</strong> the<br />
m<strong>in</strong>ds of surgeons and physicians <strong>in</strong>volved <strong>in</strong> patients care. These techniques allow us to do <strong>in</strong>terventions<br />
with greater success and high quality of care. This requires the use of robots, reduc<strong>in</strong>g access<br />
po<strong>in</strong>ts to the abdom<strong>in</strong>al cavity till one s<strong>in</strong>gle <strong>in</strong>cision or a natural orifice (LESS, NOTES). Meanwhile,<br />
progress <strong>in</strong> radiological imag<strong>in</strong>g techniques provide us with powerful diagnostic tools. The use of software<br />
such as OsiriX helped the cl<strong>in</strong>ician to br<strong>in</strong>g <strong>3D</strong> reconstructions directly to the bedside or <strong>in</strong> the<br />
operat<strong>in</strong>g room.<br />
Methods: The idea beh<strong>in</strong>d augmented reality is to challenge conventional standards to which we are<br />
used to and elaborate new tools for the modern cl<strong>in</strong>ician. Instead of try<strong>in</strong>g to put more real-world <strong>in</strong>formation<br />
<strong>in</strong> the virtual world <strong>in</strong> order to make them <strong>in</strong>teract, we pa<strong>in</strong>ted our real world, the patient, with<br />
images developed <strong>in</strong> the virtual world. For this, we therefore reconstructed from simple CT scan <strong>3D</strong><br />
images us<strong>in</strong>g the open source OsiriX software (fig.1). With a beamer attached to the operat<strong>in</strong>g table,<br />
we then projected these images on the patient surface, <strong>in</strong> the operat<strong>in</strong>g room (fig. 2-3). This gave us<br />
real-time <strong>in</strong>formation about patient anatomy, pathology and possible anatomic variations. The <strong>in</strong>struments<br />
for <strong>in</strong>tervention could be placed accord<strong>in</strong>gly to the images superimposed to the patient, thus<br />
facilitat<strong>in</strong>g the operation (fig. 4). The surgeon himself can with a remote control change the type of<br />
projection and his depth, show<strong>in</strong>g different structures at different moments of the operation.<br />
Results: The operation can be conducted with a new degree of perception provided by the superimposition<br />
of the virtual and real world.<br />
Conclusion: The purpose of this technique is an <strong>in</strong>creas<strong>in</strong>gly accurate <strong>in</strong>teraction of the projected virtual<br />
<strong>in</strong>formation with the one <strong>in</strong> our real world. Ultimately we will have a dynamic synchronous association<br />
between the projected virtual image and the real structure manipulated by the surgeon, allow<strong>in</strong>g<br />
realization of gestures such as the resection of precise structures with<strong>in</strong> solid <strong>org</strong>ans like metastases<br />
with<strong>in</strong> the liver, with more precision and m<strong>in</strong>imally <strong>in</strong>vasive techniques.<br />
Figure 1













