

2008 Clinical Practice Guidelines - Canadian Diabetes Association
2008 Clinical Practice Guidelines - Canadian Diabetes Association
2008 Clinical Practice Guidelines - Canadian Diabetes Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>2008</strong> CLINICAL PRACTICE GUIDELINES<br />
S168<br />
<strong>Diabetes</strong> and Pregnancy<br />
<strong>Canadian</strong> <strong>Diabetes</strong> <strong>Association</strong> <strong>Clinical</strong> <strong>Practice</strong> <strong>Guidelines</strong> Expert Committee<br />
The initial draft of this chapter was prepared by David Thompson MD FRCPC, Sarah Capes MD<br />
MSc FRCPC, Denice S. Feig MD MSc FRCPC,Tina Kader MD FRCPC CDE, Erin Keely MD FRCPC,<br />
Sharon Kozak BSN and Edmond A. Ryan MD FRCPC<br />
KEY MESSAGES<br />
Pregestational diabetes<br />
• All women with pre-existing type 1 or type 2 diabetes<br />
should receive preconception care to optimize glycemic<br />
control, assess complications, review medications and<br />
begin folate supplementation.<br />
• Care by an interdisciplinary diabetes healthcare team<br />
composed of diabetes nurse educators, dietitians, obstetricians<br />
and endocrinologists, both prior to conception<br />
and during pregnancy, has been shown to minimize<br />
maternal and fetal risks in women with pre-existing<br />
type 1 or type 2 diabetes.<br />
Gestational diabetes mellitus (GDM)<br />
• The suggested screening test for GDM is the<br />
Gestational <strong>Diabetes</strong> Screen – a 50-g glucose load<br />
followed by a plasma glucose test measured 1 h later.<br />
• Untreated GDM leads to increased maternal and perinatal<br />
morbidity, while intensive treatment is associated<br />
with outcomes similar to control populations.<br />
INTRODUCTION<br />
This chapter covers both pregnancy in pre-existing diabetes<br />
(pregestational diabetes) and gestational diabetes; as outlined<br />
in the text that follows, some of the management principles<br />
are common to all types of diabetes in pregnancy, including<br />
monitoring and lifestyle factors.<br />
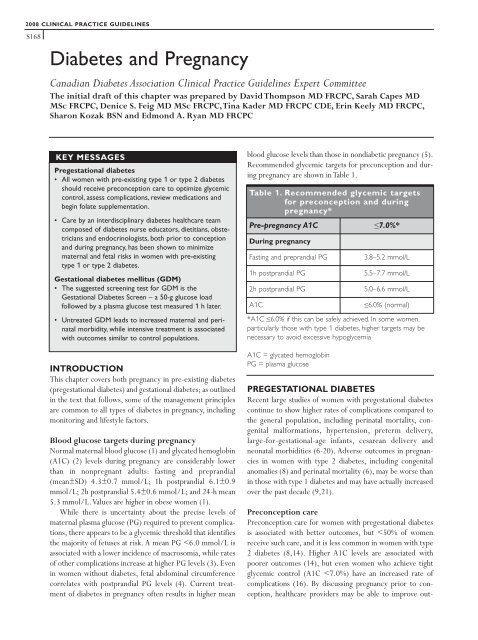
Blood glucose targets during pregnancy<br />
Normal maternal blood glucose (1) and glycated hemoglobin<br />
(A1C) (2) levels during pregnancy are considerably lower<br />
than in nonpregnant adults: fasting and preprandial<br />
(mean±SD) 4.3±0.7 mmol/L; 1h postprandial 6.1±0.9<br />
mmol/L; 2h postprandial 5.4±0.6 mmol/L; and 24-h mean<br />
5.3 mmol/L.Values are higher in obese women (1).<br />
While there is uncertainty about the precise levels of<br />
maternal plasma glucose (PG) required to prevent complications,<br />
there appears to be a glycemic threshold that identifies<br />
the majority of fetuses at risk. A mean PG








