

2008 Clinical Practice Guidelines - Canadian Diabetes Association
2008 Clinical Practice Guidelines - Canadian Diabetes Association
2008 Clinical Practice Guidelines - Canadian Diabetes Association

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>2008</strong> CLINICAL PRACTICE GUIDELINES<br />
S54<br />
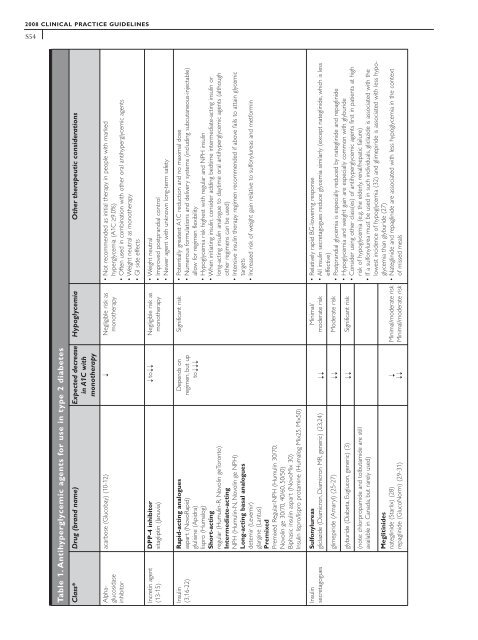
Table 1. Antihyperglycemic agents for use in type 2 diabetes<br />
Hypoglycemia Other therapeutic considerations<br />
Class* Drug (brand name) Expected decrease<br />
in A1C with<br />
monotherapy<br />
• Not recommended as initial therapy in people with marked<br />
hyperglycemia (A1C ≥9.0%)<br />
• Often used in combination with other oral antihyperglycemic agents<br />
• Weight neutral as monotherapy<br />
• GI side effects<br />
acarbose (Glucobay) (10-12) Negligible risk as<br />
monotherapy<br />
➝<br />
Alphaglucosidase<br />
inhibitor<br />
• Weight neutral<br />
• Improved postprandial control<br />
• Newer agent with unknown long-term safety<br />
to Negligible risk as<br />
monotherapy<br />
➝<br />
➝<br />
DPP-4 inhibitor<br />
sitagliptin (Januvia)<br />
Incretin agent<br />
(13-15)<br />
Significant risk • Potentially greatest A1C reduction and no maximal dose<br />
• Numerous formulations and delivery systems (including subcutaneous-injectable)<br />
allow for regimen flexibility<br />
• Hypoglycemia risk highest with regular and NPH insulin<br />
• When initiating insulin, consider adding bedtime intermediate-acting insulin or<br />
long-acting insulin analogue to daytime oral antihyperglycemic agents (although<br />
other regimens can be used)<br />
• Intensive insulin therapy regimen recommended if above fails to attain glycemic<br />
targets<br />
• Increased risk of weight gain relative to sulfonylureas and metformin<br />
Depends on<br />
regimen, but up<br />
to<br />
Rapid-acting analogues<br />
aspart (NovoRapid)<br />
glulisine (Apidra)<br />
lispro (Humalog)<br />
Short-acting<br />
regular (Humulin-R, Novolin geToronto)<br />
Intermediate-acting<br />
NPH (Humulin-N, Novolin ge NPH)<br />
Long-acting basal analogues<br />
detemir (Levemir)<br />
glargine (Lantus)<br />
Premixed<br />
Premixed Regular-NPH (Humulin 30/70;<br />
Novolin ge 30/70, 40/60, 50/50)<br />
Biphasic insulin aspart (NovoMix 30)<br />
Insulin lispro/lispro protamine (Humalog Mix25, Mix50)<br />
Insulin<br />
(3,16-22)<br />
➝<br />
• Relatively rapid BG-lowering response<br />
• All insulin secretagogues reduce glycemia similarly (except nateglinide, which is less<br />
effective)<br />
• Postprandial glycemia is especially reduced by nateglinide and repaglinide<br />
• Hypoglycemia and weight gain are especially common with glyburide<br />
• Consider using other class(es) of antihyperglycemic agents first in patients at high<br />
risk of hypoglycemia (e.g. the elderly, renal/hepatic failure)<br />
• If a sulfonylurea must be used in such individuals, gliclazide is associated with the<br />
lowest incidence of hypoglycemia (32) and glimepiride is associated with less hypoglycemia<br />
than glyburide (27)<br />
• Nateglinide and repaglinide are associated with less hypoglycemia in the context<br />
of missed meals<br />
Minimal/<br />
moderate risk<br />
Sulfonylureas<br />
gliclazide (Diamicron, Diamicron MR, generic) (23,24)<br />
Insulin<br />
secretagogues<br />
glimepiride (Amaryl) (25-27) Moderate risk<br />
glyburide (Diabeta, Euglucon, generic) (3) Significant risk<br />
➝ ➝ ➝ ➝ ➝<br />
(note: chlorpropamide and tolbutamide are still<br />
available in Canada, but rarely used)<br />
Minimal/moderate risk<br />
Minimal/moderate risk<br />
➝ ➝<br />
Meglitinides<br />
nateglinide (Starlix) (28)<br />
repaglinide (GlucoNorm) (29-31)








