Moving forward in Zimbabwe - Brooks World Poverty Institute - The ...
Moving forward in Zimbabwe - Brooks World Poverty Institute - The ...
Moving forward in Zimbabwe - Brooks World Poverty Institute - The ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Mov<strong>in</strong>g</strong> <strong>forward</strong> <strong>in</strong> <strong>Zimbabwe</strong><br />
Reduc<strong>in</strong>g poverty and promot<strong>in</strong>g growth<br />
Vacancy status: December 2007<br />
Category<br />
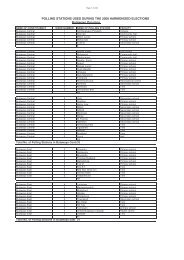
Table 7.6: Staff<strong>in</strong>g situation <strong>in</strong> the M<strong>in</strong>istry of Health and Child Welfare, 2005-2007.<br />
Required<br />
Personnel<br />
In Post<br />
2005<br />
% Vacant<br />
Posts<br />
In Post<br />
2006<br />
% Vacant<br />
Posts<br />
In Post<br />
2007<br />
Top Management 74 10 86% 7 91% 14 81%<br />
% Vacant<br />
Posts<br />
Doctors 1,761 695 61% 668 62% 667 62%<br />
Nurses 19,338 13,078 32% 13,495 30% 14,768 24%<br />
Environmental Health Department 2,395 1,217 49% 1,293 46% 1,220 49%<br />
Pharmacy 578 336 42% 338 42% 318 45%<br />
Radiography 459 140 69% 158 66% 154 66%<br />
Laboratory 631 293 54% 324 49% 320 49%<br />
Adm<strong>in</strong>istration 5,759 4,950 14% 4,960 14% 4,960 14%<br />
Records and Information 416 335 19% 335 19% 335 19%<br />
Programme Managers 34 8 76% 8 76% 8 76%<br />
Total for the whole M<strong>in</strong>istry of<br />
Health and Child Welfare<br />
Source: GoZ, 2008.<br />
35,668 23,552 34% 24,071 33% 25,343 29%<br />
operat<strong>in</strong>g at 24 per cent. This confirms the decl<strong>in</strong>e <strong>in</strong> national<br />
programm<strong>in</strong>g activity. <strong>The</strong>re simply was no capacity at national<br />
level to formulate and set out strategies to ensure that the limited<br />
resources were better deployed.<br />
Due to the shortage of senior staff, newly qualified doctors<br />
deployed to the districts could not receive adequate cl<strong>in</strong>ical and<br />
supportive supervision from specialist doctors. <strong>The</strong> high vacancy<br />
rates of 73 per cent amongst consultants at central hospitals<br />
affected the quality of services and tra<strong>in</strong><strong>in</strong>g programmes. <strong>The</strong><br />
high failure rate recorded amongst medical graduates <strong>in</strong> 2006 and<br />
2007 was directly attributed to the shortage of consultants, whose<br />
other responsibility is that of tra<strong>in</strong><strong>in</strong>g and supervision of health<br />
professionals. A similar situation prevailed for nurses’ tra<strong>in</strong><strong>in</strong>g. <strong>The</strong><br />
vacancy rate for tutors of 68 per cent suggests that the tra<strong>in</strong>ees<br />
were <strong>in</strong>creas<strong>in</strong>gly be<strong>in</strong>g tra<strong>in</strong>ed by <strong>in</strong>experienced and less qualified<br />
tutors, compromis<strong>in</strong>g the quality of output. A high failure rate was<br />
also experienced <strong>in</strong> the nurse tra<strong>in</strong><strong>in</strong>g schools. It is therefore clear<br />
that health-related human capital formation had hit the buffers by<br />
the time the IG took over. An overstretched, understaffed, underequipped<br />
and poorly remunerated staff attempted to provide<br />
a modicum of health care under some of the most difficult<br />
conditions.<br />
We can see from the forego<strong>in</strong>g that the IG took over a health<br />
system that was moribund. <strong>The</strong>re was:<br />
• Inadequate fund<strong>in</strong>g to support the grow<strong>in</strong>g needs of a<br />
population go<strong>in</strong>g through a protracted socio-economic<br />
crisis.<br />
• Little long-term strategic plann<strong>in</strong>g, and programm<strong>in</strong>g had<br />
given way to deal<strong>in</strong>g with relief and crisis. What little longterm<br />
programm<strong>in</strong>g existed was restricted to areas with r<strong>in</strong>gfenced<br />
fund<strong>in</strong>g, like HIV/AIDS. Although the MDGs still<br />
provided scope for long-term programm<strong>in</strong>g it was obvious,<br />
based on the two progress reports produced <strong>in</strong> 2004 and 2005,<br />
that the challenges of stick<strong>in</strong>g to long-term programm<strong>in</strong>g <strong>in</strong><br />
such a challeng<strong>in</strong>g environment rema<strong>in</strong>ed.<br />
• Deteriorat<strong>in</strong>g <strong>in</strong>frastructure, equipment and supplies. <strong>The</strong>se<br />
had decl<strong>in</strong>ed drastically up to the po<strong>in</strong>t that the service barely<br />
functioned.<br />
• Inadequate primary care provision<strong>in</strong>g. This had all but<br />
collapsed, especially <strong>in</strong> rural areas, and what little activity<br />
rema<strong>in</strong>ed was <strong>in</strong> the upper tiers that survived <strong>in</strong> some of the<br />
major urban centres, especially organised around surviv<strong>in</strong>g<br />
programme areas like HIV/AIDS, funded by ESP and the<br />
Global Fund.<br />
• Reduced state capacity to provide healthcare for its citizens.<br />
Church and missionary organisations have emerged once<br />
more as significant actors <strong>in</strong> health provision<strong>in</strong>g as state<br />
health facilities decl<strong>in</strong>ed.<br />
• An <strong>in</strong>creas<strong>in</strong>g frequency of epidemics (e.g. cholera, malaria),<br />
which contributed to a high burden of disease on a<br />
compromised health system.<br />
• An <strong>in</strong>creas<strong>in</strong>g level of non-communicable diseases.<br />
• An <strong>in</strong>crease <strong>in</strong> the crude death rate, ma<strong>in</strong>ly due to a fail<strong>in</strong>g<br />
health care system.<br />
• A static or worsen<strong>in</strong>g gap between the level of health <strong>in</strong><br />
urban and rural areas.<br />
Faced with these challenges, the IG will not only need to respond<br />
to these with speed but also sequentially if the health sector is<br />
to be stabilised. A key advantage of <strong>Zimbabwe</strong>’s health sector is<br />
the fact that it was decentralised. This allowed community-based<br />
programm<strong>in</strong>g to cont<strong>in</strong>ue. Unlike other post-conflict situations,<br />
where community-based programm<strong>in</strong>g collapsed, <strong>in</strong> <strong>Zimbabwe</strong><br />
structures built around the response to HIV/AIDS helped ma<strong>in</strong>ta<strong>in</strong><br />
local-level programm<strong>in</strong>g and avoided complete dis<strong>in</strong>tegration<br />
of <strong>in</strong>stitutions. Moreover, through support of donors and other<br />
partners like the Centers for Disease Control and Prevention,<br />
disease surveillance never really ceased. This aspect became crucial<br />
dur<strong>in</strong>g the outbreak of cholera as <strong>in</strong>ternational partners were able<br />
92