programma & abstracts - Nederlandse Vereniging voor Radiologie
programma & abstracts - Nederlandse Vereniging voor Radiologie
programma & abstracts - Nederlandse Vereniging voor Radiologie

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
RC<br />
<strong>programma</strong> <strong>abstracts</strong> & <strong>abstracts</strong><br />
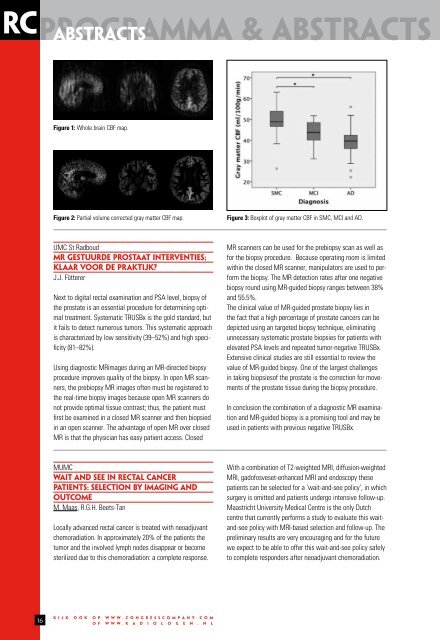
Figure 1: Whole brain CBF map.<br />
Figure 2: Partial volume corrected gray matter CBF map.<br />
Figure 3: Boxplot of gray matter CBF in SMC, MCI and AD.<br />
UMC St Radboud<br />
MR GESTUURDE PROSTAAT INTERVENTIES;<br />
KLAAR VOOR DE PRAKTIJK?<br />
J.J. Fütterer<br />
Next to digital rectal examination and PSA level, biopsy of<br />
the prostate is an essential procedure for determining optimal<br />
treatment. Systematic TRUSBx is the gold standard, but<br />
it fails to detect numerous tumors. This systematic approach<br />
is characterized by low sensitivity (39–52%) and high specificity<br />
(81–82%).<br />
Using diagnostic MRimages during an MR-directed biopsy<br />
procedure improves quality of the biopsy. In open MR scanners,<br />
the prebiopsy MR images often must be registered to<br />
the real-time biopsy images because open MR scanners do<br />
not provide optimal tissue contrast; thus, the patient must<br />
first be examined in a closed MR scanner and then biopsied<br />
in an open scanner. The advantage of open MR over closed<br />
MR is that the physician has easy patient access. Closed<br />
MR scanners can be used for the prebiopsy scan as well as<br />
for the biopsy procedure. Because operating room is limited<br />
within the closed MR scanner, manipulators are used to perform<br />
the biopsy. The MR detection rates after one negative<br />
biopsy round using MR-guided biopsy ranges between 38%<br />
and 55.5%.<br />
The clinical value of MR-guided prostate biopsy lies in<br />
the fact that a high percentage of prostate cancers can be<br />
depicted using an targeted biopsy technique, eliminating<br />
unnecessary systematic prostate biopsies for patients with<br />
elevated PSA levels and repeated tumor-negative TRUSBx.<br />
Extensive clinical studies are still essential to review the<br />
value of MR-guided biopsy. One of the largest challenges<br />
in taking biopsiesof the prostate is the correction for movements<br />
of the prostate tissue during the biopsy procedure.<br />
In conclusion the combination of a diagnostic MR examination<br />
and MR-guided biopsy is a promising tool and may be<br />
used in patients with previous negative TRUSBx.<br />
MUMC<br />
WAIT AND SEE IN RECTAL CANCER<br />
PATIENTS: SELECTION BY IMAGING AND<br />
OUTCOME<br />
M. Maas, R.G.H. Beets-Tan<br />
Locally advanced rectal cancer is treated with neoadjuvant<br />
chemoradiation. In approximately 20% of the patients the<br />
tumor and the involved lymph nodes disappear or become<br />
sterilized due to this chemoradiation: a complete response.<br />
With a combination of T2-weighted MRI, diffusion-weighted<br />
MRI, gadofosveset-enhanced MRI and endoscopy these<br />
patients can be selected for a ‘wait-and-see policy’, in which<br />
surgery is omitted and patients undergo intensive follow-up.<br />
Maastricht University Medical Centre is the only Dutch<br />
centre that currently performs a study to evaluate this waitand-see<br />
policy with MRI-based selection and follow-up. The<br />
preliminary results are very encouraging and for the future<br />
we expect to be able to offer this wait-and-see policy safely<br />
to complete responders after neoadjuvant chemoradiation.<br />
16<br />
k i j k o o k o p w w w . c o n g r e s s c o m p a n y . c o m<br />
o f w w w . r a d i o l o g e n . n l