The eligibility and enrollment rules for the U
The eligibility and enrollment rules for the U
The eligibility and enrollment rules for the U

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
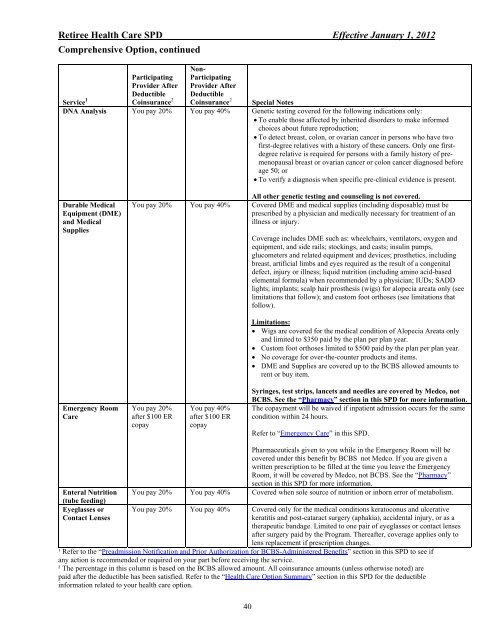
Retiree Health Care SPD Effective January 1, 2012<br />
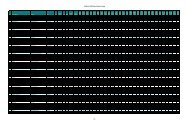
Comprehensive Option, continued<br />
Service 1<br />
Participating<br />
Provider After<br />
Deductible<br />
Coinsurance 2<br />
DNA Analysis You pay 20%<br />
Durable Medical<br />
Equipment (DME)<br />
<strong>and</strong> Medical<br />
Supplies<br />
Emergency Room<br />
Care<br />
Non-<br />
Participating<br />
Provider After<br />
Deductible<br />
Coinsurance 2 Special Notes<br />
You pay 40% Genetic testing covered <strong>for</strong> <strong>the</strong> following indications only:<br />
• To enable those affected by inherited disorders to make in<strong>for</strong>med<br />
choices about future reproduction;<br />
• To detect breast, colon, or ovarian cancer in persons who have two<br />
first-degree relatives with a history of <strong>the</strong>se cancers. Only one firstdegree<br />
relative is required <strong>for</strong> persons with a family history of premenopausal<br />
breast or ovarian cancer or colon cancer diagnosed be<strong>for</strong>e<br />
age 50; or<br />
• To verify a diagnosis when specific pre-clinical evidence is present.<br />
You pay 20% You pay 40%<br />
All o<strong>the</strong>r genetic testing <strong>and</strong> counseling is not covered.<br />
Covered DME <strong>and</strong> medical supplies (including disposable) must be<br />
prescribed by a physician <strong>and</strong> medically necessary <strong>for</strong> treatment of an<br />
illness or injury.<br />
You pay 20%<br />
after $100 ER<br />
copay<br />
You pay 40%<br />
after $100 ER<br />
copay<br />
Coverage includes DME such as: wheelchairs, ventilators, oxygen <strong>and</strong><br />
equipment, <strong>and</strong> side rails; stockings, <strong>and</strong> casts; insulin pumps,<br />
glucometers <strong>and</strong> related equipment <strong>and</strong> devices; pros<strong>the</strong>tics, including<br />
breast, artificial limbs <strong>and</strong> eyes required as <strong>the</strong> result of a congenital<br />
defect, injury or illness; liquid nutrition (including amino acid-based<br />
elemental <strong>for</strong>mula) when recommended by a physician; IUDs; SADD<br />
lights; implants; scalp hair pros<strong>the</strong>sis (wigs) <strong>for</strong> alopecia areata only (see<br />
limitations that follow); <strong>and</strong> custom foot orthoses (see limitations that<br />
follow).<br />
Limitations:<br />
• Wigs are covered <strong>for</strong> <strong>the</strong> medical condition of Alopecia Areata only<br />
<strong>and</strong> limited to $350 paid by <strong>the</strong> plan per plan year.<br />
• Custom foot orthoses limited to $500 paid by <strong>the</strong> plan per plan year.<br />
• No coverage <strong>for</strong> over-<strong>the</strong>-counter products <strong>and</strong> items.<br />
• DME <strong>and</strong> Supplies are covered up to <strong>the</strong> BCBS allowed amounts to<br />
rent or buy item.<br />
Syringes, test strips, lancets <strong>and</strong> needles are covered by Medco, not<br />
BCBS. See <strong>the</strong> “Pharmacy” section in this SPD <strong>for</strong> more in<strong>for</strong>mation.<br />
<strong>The</strong> copayment will be waived if inpatient admission occurs <strong>for</strong> <strong>the</strong> same<br />
condition within 24 hours.<br />
Refer to “Emergency Care” in this SPD.<br />
Enteral Nutrition<br />
(tube feeding)<br />
You pay 20% You pay 40%<br />
Pharmaceuticals given to you while in <strong>the</strong> Emergency Room will be<br />
covered under this benefit by BCBS not Medco. If you are given a<br />
written prescription to be filled at <strong>the</strong> time you leave <strong>the</strong> Emergency<br />
Room, it will be covered by Medco, not BCBS. See <strong>the</strong> “Pharmacy”<br />
section in this SPD <strong>for</strong> more in<strong>for</strong>mation.<br />
Covered when sole source of nutrition or inborn error of metabolism.<br />
Eyeglasses or You pay 20% You pay 40% Covered only <strong>for</strong> <strong>the</strong> medical conditions keratoconus <strong>and</strong> ulcerative<br />
Contact Lenses<br />
keratitis <strong>and</strong> post-cataract surgery (aphakia), accidental injury, or as a<br />
<strong>the</strong>rapeutic b<strong>and</strong>age. Limited to one pair of eyeglasses or contact lenses<br />
after surgery paid by <strong>the</strong> Program. <strong>The</strong>reafter, coverage applies only to<br />
lens replacement if prescription changes.<br />
¹ Refer to <strong>the</strong> “Preadmission Notification <strong>and</strong> Prior Authorization <strong>for</strong> BCBS-Administered Benefits” section in this SPD to see if<br />
any action is recommended or required on your part be<strong>for</strong>e receiving <strong>the</strong> service.<br />
² <strong>The</strong> percentage in this column is based on <strong>the</strong> BCBS allowed amount. All coinsurance amounts (unless o<strong>the</strong>rwise noted) are<br />
paid after <strong>the</strong> deductible has been satisfied. Refer to <strong>the</strong> “Health Care Option Summary” section in this SPD <strong>for</strong> <strong>the</strong> deductible<br />
in<strong>for</strong>mation related to your health care option.<br />
40