<strong>Situation</strong> <strong>analySiS</strong> of Children in uganda 20153.3.3 HIV and AIDSUganda has achieved a remarkable reduction in new HIV infections among children.Numbers have gone down from 27,660 in 2011 to 9,629 in 2013, thus achieving the NationalPriority Action Plan (NPAP) target for 2013, which stood at 10,000 (UAC, 2014a). Although85% of HIV-positive mothers and 37% of exposed infants received antiretroviral therapy(ART) for the prevention of mother-to-child transmission (MTCT) (UAC, 2014b), accordingto UNAIDS projections, the number of AIDS-related orphans has increased from 223,811 in1990 to 1,380,261 in 2012 (UAC, 2014b). With the recorded successes in the eMTCT andART programmes, the country currently faces an unprecedented HIV/AIDS burden amongthe adolescent age group as a significant proportion of vertically infected children surviveand graduate into teenage years.The latest Ugandan National Household Survey (UNHS) shows that 11.3% of children inUganda are orphaned, while 38% are considered to be vulnerable (UBOS, 2014a) and,while this figure has reduced from 14.6% in 2005/06, it is nevertheless a demographicthat needs particular attention and resource allocation. In addition urban populations aredisproportionately more likely to be infected (8.7%) compared to rural residents (7%).Urban women in particular are more at risk, with prevalence rates at 10.7% vs. 7.7% inrural women (UAC, 2014a).Adolescent girls are also severely and unevenly at risk, with two-thirds of all new HIVinfections found in this section of the population. While the number of AIDS-related deathsin children aged 0–4 years decreased significantly from 100,000 between 2000 and 2012,the number of deaths in adolescents increased from less than 50,000 to over 100,000 duringthe same period (UNICEF, 2013). The 2013 estimates show that children below 15 years ofage account for 11% of all HIV cases in Uganda and HIV is now the second leading cause ofdeath among adolescents (300 deaths every day) (UNAIDS, 2014). Although HIV positivitywas lower among pregnant adolescents (3%) compared to older pregnant women (4.9%),access to ARVs was lower among the adolescent group (94%) than among older pregnantwomen (99%).It is estimated that 18% of new HIV infections are due to mother-to-child transmission (MoH,2013b). The Government is therefore rapidly rolling out revised WHO guidelines to ensurethat HIV-infected mothers and their babies receive triple ARV prophylaxis during labourand throughout breastfeeding, and that mothers continue treatment for life (MoH, 2013b).Coverage of HIV-positive pregnant mothers accessing the package of eMTCT services nowstands at 85% (MoH, 2014c). Thirty-three districts have full coverage. However, over half ofpregnant women in four districts (Mayuge, Kaabong, otuke and Abim) who were identifiedas HIV-positive did not receive ART for the prevention of MCTC and only in 29% of districtsdid all pregnant women identified as HIV-positive receive ART for the prevention of MCTC(MoH, 2014c – see Appendix 2). MTCT treatment coverage has improved but the level ofunmet need is substantial, particularly among eligible children (UAC, 2014b).36 thE rIGht to SUrvIvaL
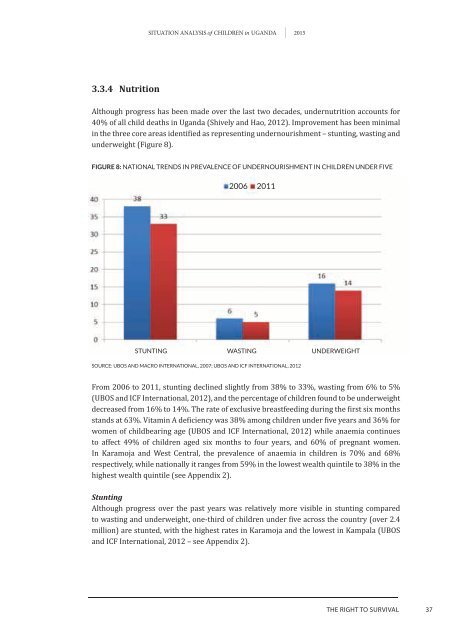
<strong>Situation</strong> <strong>analySiS</strong> of Children in uganda 20153.3.4 NutritionAlthough progress has been made over the last two decades, undernutrition accounts for40% of all child deaths in Uganda (Shively and Hao, 2012). Improvement has been minimalin the three core areas identified as representing undernourishment – stunting, wasting andunderweight (Figure 8).FIGURE 8: nAtionAl trends in prevAlence of undernourishment in children under fivesource: ubos And mAcro internAtionAl, 2007; ubos And icf internAtionAl, 2012From 2006 to 2011, stunting declined slightly from 38% to 33%, wasting from 6% to 5%(UBOS and ICF International, 2012), and the percentage of children found to be underweightdecreased from 16% to 14%. The rate of exclusive breastfeeding during the first six monthsstands at 63%. Vitamin A deficiency was 38% among children under five years and 36% forwomen of childbearing age (UBOS and ICF International, 2012) while anaemia continuesto affect 49% of children aged six months to four years, and 60% of pregnant women.In Karamoja and West Central, the prevalence of anaemia in children is 70% and 68%respectively, while nationally it ranges from 59% in the lowest wealth quintile to 38% in thehighest wealth quintile (see Appendix 2).StuntingAlthough progress over the past years was relatively more visible in stunting comparedto wasting and underweight, one-third of children under five across the country (over 2.4million) are stunted, with the highest rates in Karamoja and the lowest in Kampala (UBOSand ICF International, 2012 – see Appendix 2).thE rIGht to SUrvIvaL37