Presentation Outline ICHP Annual Meeting September 13-15
Presentation Outline ICHP Annual Meeting September 13-15
Presentation Outline ICHP Annual Meeting September 13-15

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
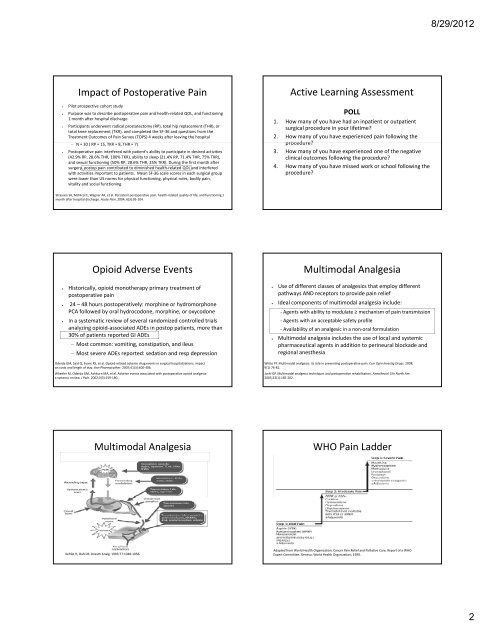
Impact of Postoperative Pain<br />
• Pilot prospective cohort study<br />
• Purpose was to describe postoperative pain and health‐related QOL, and functioning<br />
1 month after hospital discharge<br />
• Participants underwent radical prostatectomy (RP), total hip replacement (THR), or<br />
total knee replacement (TKR), and completed the SF‐36 and questions from the<br />
Treatment Outcomes of Pain Survey (TOPS) 4 weeks after leaving the hospital<br />
– N = 30 ( RP = <strong>15</strong>, TKR = 8, THR = 7) )<br />
• Postoperative pain interfered with patient's ability to participate in desired activities<br />
(42.9% RP, 28.6% THR, 100% TKR), ability to sleep (21.4% RP, 71.4% THR, 75% TKR),<br />
and sexual functioning (50% RP, 28.6% THR, 25% TKR). During the first month after<br />
surgery, postop pain contributed to diminished health‐related QOL and interfered<br />
with activities important to patients. Mean SF‐36 scale scores in each surgical group<br />
were lower than US norms for physical functioning, physical roles, bodily pain,<br />
vitality and social functioning<br />
Strassels SA, McNicol E, Wagner AK, et al. Persistent postoperative pain, health‐related quality of life, and functioning 1<br />
month after hospital discharge. Acute Pain. 2004; 6(3):95‐104.<br />
Opioid Adverse Events<br />
• Historically, opioid monotherapy primary treatment of<br />
postoperative pain<br />
• 24 –48 hours postoperatively: morphine or hydromorphone<br />
PCA followed by oral hydrocodone, morphine, or oxycodone<br />
• In a systematic review of several randomized controlled trials<br />
analyzing opioid‐associated ADEs in postop patients, more than<br />
30% of patients reported GI ADEs<br />
– Most common: vomiting, constipation, and ileus<br />
– Most severe ADEs reported: sedation and resp depression<br />
Oderda GM, Said Q, Evans RS, et al. Opioid‐related adverse drug events in surgical hospitalizations: impact<br />
on costs and length of stay. Ann Pharmacother. 2007;41(3):400‐406.<br />
Wheeler M, Oderda GM, Ashburn MA, el al. Adverse events associated with postoperative opioid analgesia:<br />
a systemic review. J Pain. 2002;3(3):<strong>15</strong>9‐180.<br />
Multimodal Analgesia<br />
Kehlet H, Dahl JB. Anesth Analg. 1993;77:1048‐1056.<br />
Active Learning Assessment<br />
POLL<br />
1. How many of you have had an inpatient or outpatient<br />
surgical procedure in your lifetime?<br />
2. How many of you have experienced pain following the<br />
procedure?<br />
3. How many of you have experienced one of the negative<br />
clinical outcomes following the procedure?<br />
4. How many of you have missed work or school following the<br />
procedure?<br />
Multimodal Analgesia<br />
• Use of different classes of analgesics that employ different<br />
pathways AND receptors to provide pain relief<br />
• Ideal components of multimodal analgesia include:<br />
‐ Agents with ability to modulate ≥ mechanism of pain transmission<br />
‐ Agents with an acceptable safety profile<br />
‐ Availability of an analgesic in a non‐oral formulation<br />
• Multimodal analgesia includes the use of local and systemic<br />
pharmaceutical agents in addition to perineural blockade and<br />
regional anesthesia<br />
White PF. Multimodal analgesia: its role in preventing postoperative pain. Curr Opin Investig Drugs. 2008;<br />
9(1):76‐82.<br />
Joshi GP. Multimodal analgesia techniques and postoperative rehabilitation. Anesthesiol Clin North Am.<br />
2005;23(1):185‐202.<br />
WHO Pain Ladder<br />
Adapted from World Health Organization. Cancer Pain Relief and Palliative Care, Report of a WHO<br />
Expert Committee. Geneva: World Health Organization; 1990.<br />
8/29/2012<br />
2