Presentation Outline ICHP Annual Meeting September 13-15
Presentation Outline ICHP Annual Meeting September 13-15
Presentation Outline ICHP Annual Meeting September 13-15

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
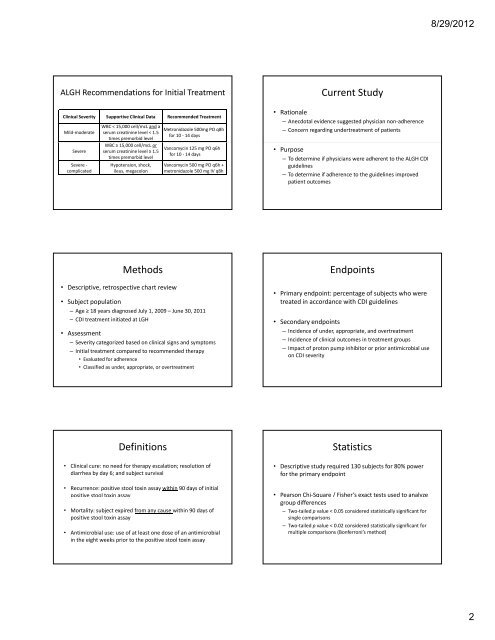
ALGH Recommendations for Initial Treatment<br />
Clinical Severity Supportive Clinical Data Recommended Treatment<br />
Mild‐moderate<br />
Severe<br />
Severe ‐<br />
complicated<br />
WBC < <strong>15</strong>,000 cell/mcL and a<br />
serum creatinine level < 1.5<br />
times premorbid level<br />
WBC ≥ <strong>15</strong>,000 cell/mcL or<br />
serum creatinine level ≥ 1.5<br />
times premorbid level<br />
Hypotension, shock,<br />
ileus, megacolon<br />
Methods<br />
• Descriptive, retrospective chart review<br />
Metronidazole 500mg PO q8h<br />
for 10 ‐ 14 days<br />
Vancomycin 125 mg PO q6h<br />
for 10 ‐ 14 days<br />
Vancomycin 500 mg PO q6h +<br />
metronidazole 500 mg IV q8h<br />
• Subject population<br />
– Age ≥ 18 years diagnosed July 1, 2009 – June 30, 2011<br />
– CDI treatment initiated at LGH<br />
• Assessment<br />
– Severity categorized based on clinical signs and symptoms<br />
– Initial treatment compared to recommended therapy<br />
• Evaluated for adherence<br />
• Classified as under, appropriate, or overtreatment<br />
Definitions<br />
• Clinical cure: no need for therapy escalation; resolution of<br />
diarrhea by day 6; and subject survival<br />
• Recurrence: positive stool toxin assay within 90 days of initial<br />
positive stool toxin assay<br />
• Mortality: subject expired from any cause within 90 days of<br />
positive stool toxin assay<br />
• Antimicrobial use: use of at least one dose of an antimicrobial<br />
in the eight weeks prior to the positive stool toxin assay<br />
Current Study<br />
• Rationale<br />
– Anecdotal evidence suggested physician non‐adherence<br />
– Concern regarding undertreatment of patients<br />
• Purpose<br />
– To determine if physicians were adherent to the ALGH CDI<br />
guidelines<br />
– To determine if adherence to the guidelines improved<br />
patient outcomes<br />
Endpoints<br />
• Primary endpoint: percentage of subjects who were<br />
treated in accordance with CDI guidelines<br />
• SSecondary d endpoints d i t<br />
– Incidence of under, appropriate, and overtreatment<br />
– Incidence of clinical outcomes in treatment groups<br />
– Impact of proton pump inhibitor or prior antimicrobial use<br />
on CDI severity<br />
Statistics<br />
• Descriptive study required <strong>13</strong>0 subjects for 80% power<br />
for the primary endpoint<br />
• Pearson Chi‐Square / Fisher’s exact tests used to analyze<br />
q / y<br />
group differences<br />
– Two‐tailed p value < 0.05 considered statistically significant for<br />
single comparisons<br />
– Two‐tailed p value < 0.02 considered statistically significant for<br />
multiple comparisons (Bonferroni’s method)<br />
8/29/2012<br />
2