- Page 2 and 3: WORLD HEALTH ORGANIZATION WHO OMS I
- Page 4 and 5: WORLD CANCER REPORT Editors Bernard
- Page 6 and 7: CONTENTS Foreword 9 1 The global bu
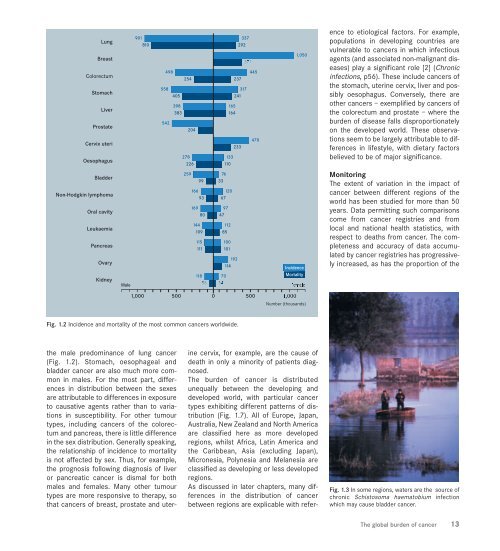
- Page 8 and 9: The global burden of cancer Cancer
- Page 12 and 13: Central and Southern Europe differ
- Page 14 and 15: Incidence of cancer in South Centra
- Page 16 and 17: from documentation of disease to a
- Page 18 and 19: TOBACCO SUMMARY >In addition to lun
- Page 20 and 21: Fig. 2.3 Smoking by children is inc
- Page 22 and 23: Cancers positively Sex Standardized
- Page 24 and 25: PHARMACOLOGICAL APPROACHES TO SMOKI
- Page 26 and 27: level the dose—response relations
- Page 28 and 29: lipoprotein-associated cholesterol,
- Page 30 and 31: Agent Cancer site/cancer Main indus
- Page 32 and 33: Industry, occupation Cancer site/ca
- Page 34 and 35: to occupational exposures in develo
- Page 36 and 37: Air pollutant WHO Air Quality Guide
- Page 38 and 39: der cancer of the order of 50% is p
- Page 40 and 41: AFLATOXIN B 1 HEPATITIS VIRUS (chro
- Page 42 and 43: Fig. 2.30 Correlation between regio
- Page 44 and 45: MEDICINAL DRUGS SUMMARY > Certain d
- Page 46 and 47: Drug or drug combination Cancer IAR
- Page 48 and 49: Agent or substance Cancer site/canc
- Page 50 and 51: sources of electromagnetic fields [
- Page 52 and 53: CHRONIC INFECTIONS SUMMARY > Infect
- Page 54 and 55: Infection Subclinical Mutagenic fac
- Page 56 and 57: TUMOURS ASSOCIATED WITH HIV/AIDS Ap
- Page 58 and 59: DIET AND NUTRITION SUMMARY > Up to
- Page 60 and 61:
Fig. 2.54 The age-adjusted mortalit
- Page 62 and 63:
OVERWEIGHT, OBESITY AND PHYSICAL AC
- Page 64 and 65:
IMMUNOSUPPRESSION SUMMARY >Persiste
- Page 66 and 67:
Fig. 2.64 Cancer following immunosu
- Page 68 and 69:
Syndrome Gene Location Cancer site/
- Page 70 and 71:
viduals, confirmation of a gene def
- Page 72 and 73:
REPRODUCTIVE FACTORS AND HORMONES S
- Page 74 and 75:
PHYTO-ESTROGENS AND CANCER PEVENTIO
- Page 76 and 77:
Indicator Number of oral contracept
- Page 79 and 80:
Mechanisms of tumour development Th
- Page 81 and 82:
The stages in tumorigenesis have be
- Page 83 and 84:
PRECURSOR LESIONS IN CHEMOPREVENTIO
- Page 85 and 86:
CARCINOGEN ACTIVATION AND DNA REPAI
- Page 87 and 88:
adducts, a few weeks or months for
- Page 89 and 90:
I Reactive oxygen species Methylati
- Page 91 and 92:
which remove the mismatched bases,
- Page 93 and 94:
Common human oncogenes Many common
- Page 95 and 96:
product of the RB1 gene (pRb) and a
- Page 97 and 98:
ates a molecular bridge between p53
- Page 99 and 100:
potential cancer genes altered thro
- Page 101 and 102:
One of the earliest genes to be ide
- Page 103 and 104:
Regulation of the cell cycle and co
- Page 105 and 106:
CELL-CELL COMMUNICATION SUMMARY > C
- Page 107 and 108:
Connexin genes and tumour suppressi
- Page 109 and 110:
APOPTOSIS SUMMARY > The term apopto
- Page 111 and 112:
Caspase-8 Caspase-3 c-FLIP Procaspa
- Page 113 and 114:
ways. Several options are under inv
- Page 115 and 116:
INVASION AND METASTASIS SUMMARY > T
- Page 117 and 118:
laminin, entactin and also heparan
- Page 119 and 120:
Target Example of agent Comments Ad
- Page 121 and 122:
organs, and to respond to local gro
- Page 123 and 124:
TOBACCO CONTROL SUMMARY > Tobacco-i
- Page 125 and 126:
Region Deaths due to % of total dea
- Page 127 and 128:
ipated, is primarily attributable t
- Page 129 and 130:
smoke. This may be achieved in part
- Page 131 and 132:
there is no evidence for the effica
- Page 133 and 134:
industries, processes and occupatio
- Page 135 and 136:
stoves arises in rural areas of dev
- Page 137 and 138:
Climbing plants on trellis at end r
- Page 139 and 140:
HEPATITIS B VACCINATION SUMMARY > P
- Page 141 and 142:
Fig. 4.17 Chronic active HBV-associ
- Page 143 and 144:
HUMAN PAPILLOMAVIRUS VACCINATION SU
- Page 145 and 146:
Vaccine Site of trial Number of pat
- Page 147 and 148:
prolonged use. Similar drugs, that
- Page 149 and 150:
aspirin and other non-steroidal ant
- Page 151 and 152:
SCREENING FOR BREAST CANCER SUMMARY
- Page 153 and 154:
Fig. 4.35 Cumulative mortality from
- Page 155 and 156:
SCREENING FOR PROSTATE CANCER SUMMA
- Page 157 and 158:
Fig. 4.39 Poster designed for an an
- Page 159 and 160:
is around 10% for cancer (out of ev
- Page 161 and 162:
45 with one positive rehydrated FOB
- Page 163 and 164:
eing based on (i) time trends in th
- Page 165 and 166:
Fig. 4.48 Women at a clinic in Indi
- Page 167 and 168:
SCREENING FOR ORAL CANCER SUMMARY >
- Page 169 and 170:
India will provide useful informati
- Page 171 and 172:
cer incidence following cure of inf
- Page 173 and 174:
100 50 25 10 5 2.5 1 Japan Males Fe
- Page 175 and 176:
Human cancers by organ site Maligna
- Page 177 and 178:
tobacco smoking: age at start, aver
- Page 179 and 180:
diagnosis is usually confirmed by h
- Page 181 and 182:
is frequent and survival rates are
- Page 183 and 184:
Fig. 5.14 Physician reading digital
- Page 185 and 186:
Markers of prognosis in breast canc
- Page 187 and 188:
cer in the contralateral breast (Ch
- Page 189 and 190:
100 50 25 10 5 2.5 1 Japan Chile Po
- Page 191 and 192:
depends on staging. Small intramuco
- Page 193 and 194:
Fig. 5.30 A diet rich in fresh frui
- Page 195 and 196:
ane protein involved in cell adhesi
- Page 197 and 198:
LIVER CANCER SUMMARY > About 560,00
- Page 199 and 200:
Fig. 5.39 A woman in the Gambia pre
- Page 201 and 202:
REFERENCES 1. Ferlay J, Bray F, Par
- Page 203 and 204:
Certain Possible Uncertain Age Andr
- Page 205 and 206:
Management The dramatic division be
- Page 207 and 208:
TUMOUR NORMAL Gastrula PGC 2n Impri
- Page 209 and 210:
CANCERS OF THE FEMALE REPRODUCTIVE
- Page 211 and 212:
Fig. 5.62 Five-year relative surviv
- Page 213 and 214:
Inheritance of high-penetrance gene
- Page 215 and 216:
invasive malignant. Malignant germ
- Page 217 and 218:
OESOPHAGEAL CANCER SUMMARY >Cancer
- Page 219 and 220:
Fig. 5.76 A radiographic view of an
- Page 221 and 222:
with a stent; laser recannulation,
- Page 223 and 224:
Fig. 5.82 Risk of bladder cancer am
- Page 225 and 226:
Partial cystectomy is appropriate f
- Page 227 and 228:
poorly known since hypopharyngeal c
- Page 229 and 230:
Fig. 5.92 Oral leukoplakia with mil
- Page 231 and 232:
LYMPHOMA SUMMARY > Malignant lympho
- Page 233 and 234:
T Fig. 5.101 Nuclear magnetic reson
- Page 235 and 236:
Fig. 5.106 Five-year relative survi
- Page 237 and 238:
Fig. 5.109 The immediate aftermath
- Page 239 and 240:
A B Fig. 5.113 Acute myeloid leukae
- Page 241 and 242:
Fig. 5.118 Five-year relative survi
- Page 243 and 244:
Fig. 5.120 Age-specific incidence a
- Page 245 and 246:
Hereditary condition Mode of inheri
- Page 247 and 248:
MELANOMA SUMMARY > Approximately 13
- Page 249 and 250:
Fig. 5.131 Primary melanoma with a
- Page 251 and 252:
THYROID CANCER SUMMARY > Cancer of
- Page 253 and 254:
Papillary carcinoma RET/PTC TRK BRA
- Page 255 and 256:
KIDNEY CANCER SUMMARY > Cancer of t
- Page 257 and 258:
Stage Clear cell carcinoma Papillar
- Page 259 and 260:
TUMOURS OF THE NERVOUS SYSTEM SUMMA
- Page 261 and 262:
ing the optic tract, brain stem and
- Page 263 and 264:
mut = mutant p53 wt = wildtype p53
- Page 265 and 266:
SURGICAL ONCOLOGY SUMMARY > Surgica
- Page 267 and 268:
Year Radical mastectomy (%) Modifie
- Page 269 and 270:
TELEMEDICINE The prospects for tele
- Page 271 and 272:
Equipment Energy 50% depth dose App
- Page 273 and 274:
CANCER EDUCATION IN MEDICAL COURSES
- Page 275 and 276:
Fig. 6.10 Crystals of cisplatin: mo
- Page 277 and 278:
Responsiveness Cancer (in decreasin
- Page 279 and 280:
Most of the world’s most common c
- Page 281 and 282:
treatment of cancer. The problems l
- Page 283 and 284:
duction. It is clear that tumour ce
- Page 285 and 286:
REHABILITATION SUMMARY > Rehabilita
- Page 287 and 288:
cer and its associated disability.
- Page 289 and 290:
REFERENCES 1. Garden FH, Gillis TA
- Page 291 and 292:
Cancer pain relief varies and in so
- Page 293 and 294:
EMERGING ISSUES IN PALLIATIVE CARE
- Page 295 and 296:
Cancer control The negative impact
- Page 297 and 298:
priority to cancer control activiti
- Page 299 and 300:
Prevention of cancer Every country
- Page 301 and 302:
- Assessing the magnitude of the ca
- Page 303 and 304:
high-risk women. Further details on
- Page 305 and 306:
ecords departments are either rudim
- Page 307 and 308:
THE INTERNATIONAL AGENCY FOR RESEAR
- Page 309 and 310:
in the capitals/urban areas of four
- Page 311 and 312:
in the overall cancer strategy. WHO
- Page 313 and 314:
68% 1955 1975 1995 2025 32% 40% by
- Page 315 and 316:
Fig. 7.15 A grandfather at work in
- Page 317 and 318:
Fig. 7.17 Main causes of death in d
- Page 319 and 320:
Contributors and Reviewers Sources
- Page 321 and 322:
Dr Vera Luiz da Costa e Silva Tobac
- Page 323 and 324:
Georgia Moore Centers for Disease C
- Page 325 and 326:
REVIEWERS Dr Sandra E. Brooks 405 W
- Page 327 and 328:
2.53 T. Norat and E. Riboli, IARC 2
- Page 329 and 330:
Gastroenterology, 118(2 Suppl 1): S
- Page 331 and 332:
5.106 & 5.107 IARC/SEER/Osaka Cance
- Page 333 and 334:
4.17 R. Lambert, IARC/Adapted from
- Page 335 and 336:
Brain cancer, see nervous system tu
- Page 337 and 338:
Fibroblast growth factor (FGF), 117
- Page 339 and 340:
Microarray, 240 Micronutrients, 65,
- Page 341 and 342:
S Saccharin, 64, 85 Salicin, 153 Sa