Comparison between OPD-scan results and contrast sensitivity of three intraocular lenses: spheric AcrySof SN60AT ...217INTRODUCTIONWavefront science has helped explain that this<strong>de</strong>cline occurs because of increasingspherical aberration of the human lens (1-3) ,New possibilities appeared when new technologies were<strong>de</strong>veloped, like the wavefront analysis using theHartmann-Shack aberrometer and the optical pathdifference scan (OPD-scan), which measures the distancelight travels in different paths going through the eye,measuring the optical system aberration (2,3) . Theintegration of wavefront technology and lens-basedsurgery represents a step toward improving functionalvision and the quality of life for cataract patients (2-6). Aswe have learned that the optical wavefront of the cornearemains stable throughout life, the lens has started tocome into its own as a primary locus for refractivesurgery (7) .The evolution in cataract surgery has evolved withnew surgical techniques, instrumentals, viscoelastic<strong>de</strong>vices and IOL <strong>de</strong>signs that provi<strong>de</strong> high-qualityoptical imagery at all focal distance, since the first use ofthem by Ridley (1) . What remains is a challenge for opticalscientists and material engineers to <strong>de</strong>sign a IOLs thatcompensate for any aberrations inherent in the cornea.The multifocal IOL try to minimize loss of inci<strong>de</strong>nt lightto higher or<strong>de</strong>rs of diffraction, reducing opticalaberrations, and balancing the brightness of the focusedand unfocused images (8) .In the AcrySof ® SN60D3 Restor ® IOL, the logicof placing the diffractive element centrally <strong>de</strong>pends onthe near synkinesis of convergence, accommodation, andmiosis. As the pupil constricts, the focal dominance of thelens shifts from almost purely distance to equal-parts’distance and near. This approach conserves efficiencyfor mesopic activities when the pupil is larger, such asnight driving, but reduces near vision un<strong>de</strong>r mesopicconditions (6) .Contrast sensitivity testing has confirmed a <strong>de</strong>clinein visual performance with age (6-10) . Improvements inocular biometry and cataract surgery have minimizedrefractive error, promoting quick visual recovery, withlow intraoperative complications, good postoperativequality of functional vision, more accurately <strong>de</strong>scribedon the basis of the ability to precisely discern <strong>de</strong>tailsof images regardless of lighting and brightnessconditions (7,11) .The purpose of this study is to compare theaberrometry results with OPD-scan and contrastsensitivity in patients who had implantation of theAcrySof SN60D3 multifocal IOL, the AcrySof SA60ATspheric monofocal IOL and the AcrySof SA60ATaspheric monofocal IOL in cataract surgery.METHODSThis prospective, randomized study comprised 96eyes of 48 patients selected between march 2005 andjuly 2006. This study was conducted according toestablished ethical standards for clinical research andthe internal review board of our hospital approved thestudy protocol.Inclusion criteria was age between 45 and 75 yearsold, presence of cataracts, classified by the Lens OpacitySystem II (LOCS II), and corneal astigmatism less than1.00 diopter in both groups, with no other ocularpathologies, no previous ocular surgery or use of topichipotensive medication and pupil diameter of at least 3.5mm or more un<strong>de</strong>r mesopic and photopic light conditionsas measured by the Colvard pupillometer (Oasis,Glendora). In addition, all patients with systemic diseasepotentially affecting vision or specifically affectingcontrast sensitivity, such as diabetes retinopathy, wereexclu<strong>de</strong>d. Patient with intraoperative or postoperativecomplications, including lens fixation that could not beclassified as ‘‘secure and in-the-bag’’ or lens <strong>de</strong>scentrationgreater than 0.5 mm were not inclu<strong>de</strong>d in the study.A standard ophthalmic evaluation, performed inall visits, which inclu<strong>de</strong>d distance (6m), intermediate(70cm) and near (33cm) best corrected and uncorrectedvisual acuity, biomicroscopy, intraocular pressuremeasurement and fundoscopy. The patients wererandomized, using the Randomizer ® program, into oneof three groups for IOL implantation as follows: sphericmonofocal group, AcrySof ® Natural ® (SN60AT, AlconLabs), aspheric monofocal group, AcrySof ® Natural ® WF(SN60WF, Alcon Labs) and multifocal group, AcrySof ®Restor ® (SA60D3, Alcon Labs).All patients IOL calculation were done byimmersion ultrasonic technique by single experience<strong>de</strong>xaminator (A.F.P.M.) using the Ocuscan RXP biometer(Alcon Labs), and the IOL power selected with Hoffer-Q or SRK/T formulas according to measured eye axiallength (12) . Target refraction was plano (0D), or the firstpositive value for the multifocal group and targetrefraction was plano (0D), or the first negative value for thespheric and aspheric monofocal group.Pupil diameters were Ginsburg box phtometer(85 cd/m 2 and 6 cd/m 2 ) by means of a Colvardpupillometer (Oasis, Glendora). All subjects un<strong>de</strong>rwentRev Bras Oftalmol. 2009; 68 (4): 216-22
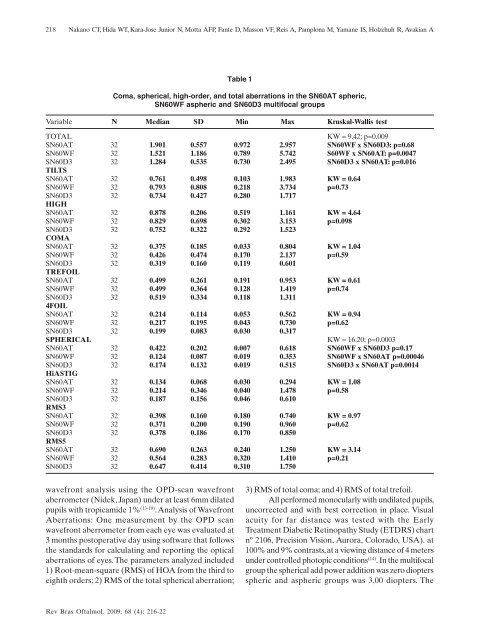
218Nakano CT, Hida WT, Kara-Jose Junior N, Motta AFP, Fante D, Masson VF, Reis A, Pamplona M, Yamane IS, Holzchuh R, Avakian ATable 1Coma, spherical, high-or<strong>de</strong>r, and total aberrations in the SN60AT spheric,SN60WF aspheric and SN60D3 multifocal groupsVariable N Median SD Min Max Kruskal-Wallis testTOTALKW = 9.42; p=0.009SN60AT 32 1.901 0.557 0.972 2.957 SN60WF x SN60D3: p=0.68SN60WF 32 1.521 1.186 0.789 5.742 S60WF x SN60AT: p=0.0047SN60D3 32 1.284 0.535 0.730 2.495 SN60D3 x SN60AT: p=0.016TILTSSN60AT 32 0.761 0.498 0.103 1.983 KW = 0.64SN60WF 32 0.793 0.808 0.218 3.734 p=0.73SN60D3 32 0.734 0.427 0.280 1.717HIGHSN60AT 32 0.878 0.206 0.519 1.161 KW = 4.64SN60WF 32 0.829 0.698 0.302 3.153 p=0.098SN60D3 32 0.752 0.322 0.292 1.523COMASN60AT 32 0.375 0.185 0.033 0.804 KW = 1.04SN60WF 32 0.426 0.474 0.170 2.137 p=0.59SN60D3 32 0.319 0.160 0.119 0.601TREFOILSN60AT 32 0.499 0.261 0.191 0.953 KW = 0.61SN60WF 32 0.499 0.364 0.128 1.419 p=0.74SN60D3 32 0.519 0.334 0.118 1.3114FOILSN60AT 32 0.214 0.114 0.053 0.562 KW = 0.94SN60WF 32 0.217 0.195 0.043 0.730 p=0.62SN60D3 32 0.199 0.083 0.030 0.317SPHERICALKW = 16.20; p=0.0003SN60AT 32 0.422 0.202 0.007 0.618 SN60WF x SN60D3 p=0.17SN60WF 32 0.124 0.087 0.019 0.353 SN60WF x SN60AT p=0.00046SN60D3 32 0.174 0.132 0.019 0.515 SN60D3 x SN60AT p=0.0014HiASTIGSN60AT 32 0.134 0.068 0.030 0.294 KW = 1.08SN60WF 32 0.214 0.346 0.040 1.478 p=0.58SN60D3 32 0.187 0.156 0.046 0.610RMS3SN60AT 32 0.398 0.160 0.180 0.740 KW = 0.97SN60WF 32 0.371 0.200 0.190 0.960 p=0.62SN60D3 32 0.378 0.186 0.170 0.850RMS5SN60AT 32 0.690 0.263 0.240 1.250 KW = 3.14SN60WF 32 0.564 0.283 0.320 1.410 p=0.21SN60D3 32 0.647 0.414 0.310 1.750wavefront analysis using the OPD-scan wavefrontaberrometer (Ni<strong>de</strong>k, Japan) un<strong>de</strong>r at least 6mm dilatedpupils with tropicami<strong>de</strong> 1% (13-19) . Analysis of WavefrontAberrations: One measurement by the OPD scanwavefront aberrometer from each eye was evaluated at3 months postoperative day using software that followsthe standards for calculating and reporting the opticalaberrations of eyes. The parameters analyzed inclu<strong>de</strong>d1) Root-mean-square (RMS) of HOA from the third toeighth or<strong>de</strong>rs; 2) RMS of the total spherical aberration;3) RMS of total coma; and 4) RMS of total trefoil.All performed monocularly with undilated pupils,uncorrected and with best correction in place. Visualacuity for far distance was tested with the EarlyTreatment Diabetic Retinopathy Study (ETDRS) chartnº 2106, Precision Vision, Aurora, Colorado, USA). at100% and 9% contrasts, at a viewing distance of 4 metersun<strong>de</strong>r controlled photopic conditions (14) . In the multifocalgroup the spherical add power addition was zero dioptersspheric and aspheric groups was 3,00 diopters. TheRev Bras Oftalmol. 2009; 68 (4): 216-22
- Page 3 and 4: 192Revista Brasileira de Oftalmolog
- Page 5 and 6: 194212 Biometria ultrassônica no c
- Page 7 and 8: 196Novidades na cirurgia de catarat
- Page 11 and 12: 200Leonor ACI, Dalfré JT, Moreira
- Page 13 and 14: 202Santhiago MR, Monica LAM, Kara-J
- Page 15 and 16: 204Santhiago MR, Monica LAM, Kara-J
- Page 17 and 18: 206ARTIGO ORIGINALPrevalência de i
- Page 19 and 20: 208Machado MO, Fraga DS, Floriano J
- Page 21 and 22: 210Machado MO, Fraga DS, Floriano J
- Page 23 and 24: 212ARTIGO ORIGINALBiometria ultrass
- Page 25 and 26: 214Martins FCR, Miyaji ME, Lima VL,
- Page 27: 216ARTIGO ORIGINALComparison betwee
- Page 31 and 32: 220Nakano CT, Hida WT, Kara-Jose Ju
- Page 33 and 34: 222Nakano CT, Hida WT, Kara-Jose Ju
- Page 35 and 36: 224Passos AF, Kiefer K, Amador RCIN
- Page 37 and 38: 226Passos AF, Kiefer K, Amador RCAF
- Page 39 and 40: 228Passos AF, Kiefer K, Amador RCde
- Page 41 and 42: 230Passos AF, Kiefer K, Amador RC32
- Page 43 and 44: 232Damasceno EF, Damasceno NAP, Cos
- Page 45 and 46: 234Damasceno EF, Damasceno NAP, Cos
- Page 47 and 48: 236Damasceno EF, Damasceno NAP, Cos
- Page 49 and 50: 238Marback EF, Pereira FF, Galvão
- Page 51 and 52: 240Marback EF, Pereira FF, Galvão
- Page 53 and 54: 242Aragão REM, Barreira IMA, Bezer
- Page 55 and 56: 244Aragão REM, Barreira IMA, Bezer
- Page 57 and 58: 246Sardinha M, Mendes Junior ES, Br
- Page 59 and 60: 248Sardinha M, Mendes Junior ES, Br
- Page 61 and 62: 250Instruções aos autoresA Revist
- Page 63: 252RevistaBrasileira deOftalmologia