

Delivering continuity of midwifery care to Queensland women
Delivering continuity of midwifery care to Queensland women
Delivering continuity of midwifery care to Queensland women

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Considerations when implementing caseload (group practice) model<br />
It is essential that if this model is under consideration it can be demonstrated:<br />
• there is a critical mass <strong>of</strong> midwives willing (or who are able <strong>to</strong> be supported) <strong>to</strong> work<br />
within such a model <strong>of</strong> <strong>care</strong><br />
• the model is self-sustaining in the face <strong>of</strong> resignations and departures from the facility<br />
(succession planning is integral)<br />
• there is support and collaboration with relevant medical colleagues such as obstetricians,<br />
general practitioners and obstetric registrars (may be <strong>of</strong>f-site support)<br />
• National Midwifery Guidelines for Consultation and Referral (ACM 2008) is unders<strong>to</strong>od by<br />
all practitioners<br />
• the clinical governance structures around the model meets the best practise requirements.<br />
Revenue for caseload (Group Practice) based on six FTE midwives<br />
—240 births per year<br />
This generalised model was constructed using inlier payments for DRGs and clinic<br />
attendances (<strong>Queensland</strong> Health 2010a) and supports the premise that a caseload<br />
<strong>midwifery</strong> model <strong>of</strong> <strong>care</strong> can be a financially viable proposition within the existing structure<br />
<strong>of</strong> a <strong>Queensland</strong> Health maternity service.<br />
Antenatal (AN):<br />
The average number <strong>of</strong> antenatal appointments a woman currently attends and is supported<br />
in the <strong>Queensland</strong> Health Personal Health Record documentation is 10. The funding<br />
available per antenatal visit is $165.<br />
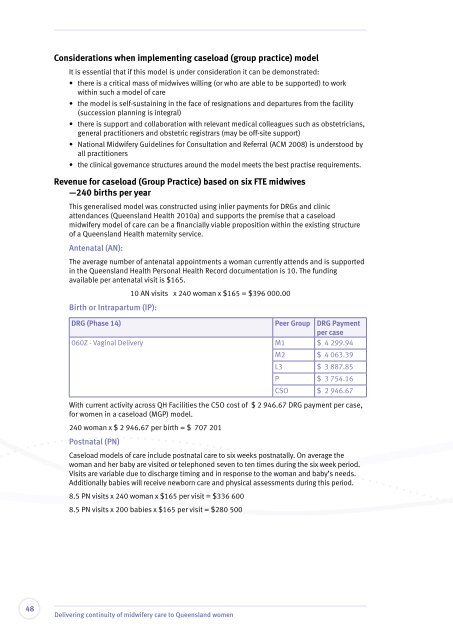
Birth or Intrapartum (IP):<br />
10 AN visits x 240 woman x $165 = $396 000.00<br />
DRG (Phase 14) Peer Group DRG Payment<br />
per case<br />
060Z - Vaginal Delivery M1 $ 4 299.94<br />
M2 $ 4 063.39<br />
L3 $ 3 887.85<br />
P $ 3 754.16<br />
CSO $ 2 946.67<br />
With current activity across QH Facilities the CSO cost <strong>of</strong> $ 2 946.67 DRG payment per case,<br />
for <strong>women</strong> in a caseload (MGP) model.<br />
240 woman x $ 2 946.67 per birth = $ 707 201<br />
Postnatal (PN)<br />
Caseload models <strong>of</strong> <strong>care</strong> include postnatal <strong>care</strong> <strong>to</strong> six weeks postnatally. On average the<br />
woman and her baby are visited or telephoned seven <strong>to</strong> ten times during the six week period.<br />
Visits are variable due <strong>to</strong> discharge timing and in response <strong>to</strong> the woman and baby’s needs.<br />
Additionally babies will receive newborn <strong>care</strong> and physical assessments during this period.<br />
8.5 PN visits x 240 woman x $165 per visit = $336 600<br />
8.5 PN visits x 200 babies x $165 per visit = $280 500<br />
48<br />
<strong>Delivering</strong> <strong>continuity</strong> <strong>of</strong> <strong>midwifery</strong> <strong>care</strong> <strong>to</strong> <strong>Queensland</strong> <strong>women</strong>













