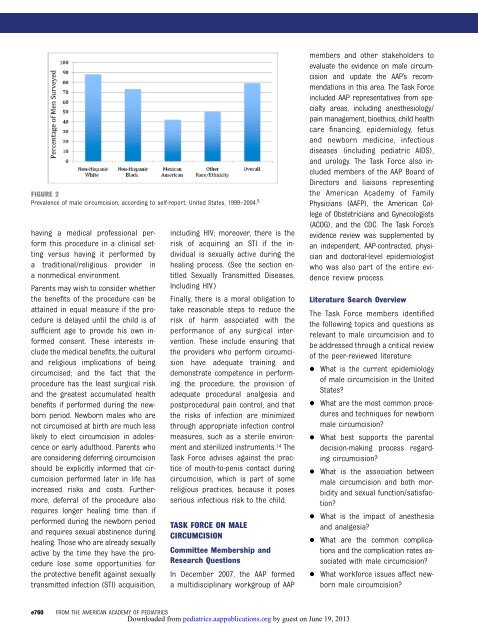
FROM THE AMERICAN ACADEMY OF PEDIATRICSFIGURE 1Incidence of in-hospital newborn male circumcision, according to data source; United States, 1999–2010. 2,3or guardians are empowered to makehealth care decisions on their behalf. 9In most situations, parents are grantedwide latitude in terms of thedecisions they make on behalf of theirchildren, and the law has respectedthose decisions except where they areclearly contrary to the best interestsof the child or place the child’s health,well-being, or life at significant risk ofserious harm. 10Parents and physicians each have anethical duty to the child to attempt tosecure the child’s best interest andwell-being. 11 Reasonable people maydisagree,however,astowhatisinthebest interest of any individual patient orhow the potential medical benefits andpotential medical harms of circumcisionshould be weighed against eachother. This situation is further c<strong>om</strong>plicatedby the fact that there are social,cultural, religious, and familial benefitsand harms to be considered as well. 12 Itis reasonable to take these nonmedicalbenefits and harms for an individualinto consideration when making a decisionabout circumcision. 13TABLE 1 Multivariate Cox Proportional Hazards Regression of Selected Factors Associated WithCircumcision Among Male Newborn Delivery Hospitalizations, United States, 1998–2005 2CharacteristicWeighted % of MaleInfant CircumcisionsAdjusted PrevalenceRate Ratios (95% CI)Hospital regionMidwest 74 3.53 (3.23–3.87)Northeast 67 2.90 (2.64–3.18)South 61 2.80 (2.56–3.07)West 30 1.00PayerPrivate 67 1.76 (1.70–1.82)Public 45 1.00Hospital locationUrban 66 1.29 (1.24–1.34)Rural 56 1.00Newborn health statusTerm, healthy 61 1.22 (1.20–1.23)Not term, healthy 54 1.00In cases such as the decision to performa circumcision in the newbornperiod (where there is reasonabledisagreement about the balance betweenmedical benefits and harms,where there are nonmedical benefitsand harms that can result fr<strong>om</strong> a decisionon whether to perform theprocedure, and where the procedureis not essential to the child’s immediatewell-being), the parents shoulddetermine what is in the best interestof the child. In the pluralistic societyof the United States, where parentsare <strong>af</strong>forded wide authority for determiningwhat constitutes appropriatechild-rearing and child welfare, itis legitimate for the parents to takeinto account their own cultural, religious,and ethnic traditions, in additionto medical factors, when makingthis choice. 11Physicians who counsel families aboutthis decision should assist parents byobjectively explaining the potentialbenefits and risks of circumcising theirinfant. 10 Becauses<strong>om</strong>efamiliesmayoptto circumcise as part of religious ortraditional practice, discussion shouldalso enc<strong>om</strong>pass risks and benefits ofPEDIATRICS Volume 130, Number 3, September 2012Downloaded fr<strong>om</strong> pediatrics.aappublications.org by guest on June 19, 2013e759
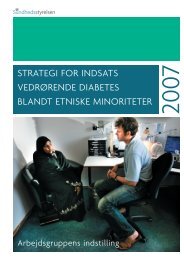
FIGURE 2Prevalence of male circumcision, according to self-report; United States, 1999–2004. 5having a medical professional performthis procedure in a clinical settingversus having it performed bya traditional/religious provider ina nonmedical environment.Parents may wish to consider whetherthe benefits of the procedure can beattained in equal measure if the procedureis delayed until the child is ofsufficient age to provide his own informedconsent. These interests includethe medical benefits; the culturaland religious implications of beingcircumcised; and the fact that theprocedure has the least surgical riskand the greatest accumulated healthbenefits if performed during the newbornperiod. Newborn males who arenot circumcised at birth are much lesslikely to elect circumcision in adolescenceor early adulthood. Parents whoare considering deferring circumcisionshould be explicitly informed that circumcisionperformed later in life hasincreased risks and costs. Furthermore,deferral of the procedure alsorequires longer healing time than ifperformed during the newborn periodand requires sexual abstinence duringhealing. Those who are already sexuallyactivebythetimetheyhavetheprocedurelose s<strong>om</strong>e opportunities forthe protective benefit against sexuallytransmitted infection (STI) acquisition,including HIV; moreover, there is therisk of acquiring an STI if the individualis sexually active during thehealing process. (See the section entitledSexually Transmitted Diseases,Including HIV.)Finally, there is a moral obligation totake reasonable steps to reduce therisk of harm associated with theperformance of any surgical intervention.These include ensuring thatthe providers who perform circumcisionhave adequate training anddemonstrate c<strong>om</strong>petence in performingthe procedure; the provision ofadequate procedural analgesia andpostprocedural pain control; and thatthe risks of infection are minimizedthrough appropriate infection controlmeasures, such as a sterile environmentand sterilized instruments. 14 TheTask Force advises against the practiceof mouth-to-penis contact duringcircumcision, which is part of s<strong>om</strong>ereligious practices, because it posesserious infectious risk to the child.TASK FORCE ON MALECIRCUMCISIONC<strong>om</strong>mittee Membership andResearch QuestionsIn December 2007, the AAP formeda multidisciplinary workgroup of AAPmembers and other stakeholders toevaluate the evidence on male circumcisionand update the AAP’s rec<strong>om</strong>mendationsin this area. The Task Forceincluded AAP representatives fr<strong>om</strong> specialtyareas, including anesthesiology/pain management, bioethics, child healthcare financing, epidemiology, fetusand newborn medicine, infectiousdiseases (including pediatric AIDS),and urology. The Task Force also includedmembers of the AAP Board ofDirectors and liaisons representingthe American Academy of FamilyPhysicians (AAFP), the American Collegeof Obstetricians and Gynecologists(ACOG), and the CDC. The Task Force’sevidence review was supplemented byan independent, AAP-contracted, physicianand doctoral-level epidemiologistwho was also part of the entire evidencereview process.Literature Search OverviewThe Task Force members identifiedthe following topics and questions asrelevant to male circumcision and tobe addressed through a critical reviewof the peer-reviewed literature: What is the current epidemiologyof male circumcision in the UnitedStates? What are the most c<strong>om</strong>mon proceduresand techniques for newbornmale circumcision? What best supports the parentaldecision-making process regardingcircumcision? What is the association betweenmale circumcision and both morbidityand sexual function/satisfaction? What is the impact of anesthesiaand analgesia? What are the c<strong>om</strong>mon c<strong>om</strong>plicationsand the c<strong>om</strong>plication rates associatedwith male circumcision? What workforce issues <strong>af</strong>fect newbornmale circumcision?e760FROM THE AMERICAN ACADEMY OF PEDIATRICSDownloaded fr<strong>om</strong> pediatrics.aappublications.org by guest on June 19, 2013
- Page 1 and 2:
OMSKÆRINGAF DRENGENotat2013
- Page 3 and 4: Indhold1 Sundhedsstyrelsens sammenf
- Page 5 and 6: 1 Sundhedsstyrelsens sammenfatningO
- Page 7 and 8: døgn under indlæggelse på sygehu
- Page 9 and 10: arnet ligger på en pude på et bor
- Page 11 and 12: se områder i Afrika. WHO understre
- Page 13 and 14: 3 Omskæring i DanmarkFor en del å
- Page 15 and 16: Hvis en person, der hverken er læg
- Page 17 and 18: 4 Omskæring i andre landEfter Sund
- Page 19 and 20: sundhedsmæssige fordele ikke er tu
- Page 21: 6 Bilagsfortegnelse:Bilag 1:Sundhed
- Page 24 and 25: WHITEPAPER- OM RITUEL OMSKÆRELSE A
- Page 26 and 27: OM RITUEL JØDISK OMSKÆRELSE AF DR
- Page 29 and 30: White Paper om religiøs omskærels
- Page 31 and 32: har været oppe med jævne mellemru
- Page 33 and 34: To tredjedel færre infektioner på
- Page 35 and 36: Der er en betydelig risiko for, at
- Page 37 and 38: 2.3 Beskrivelse af afrapporteringen
- Page 39 and 40: 3.5 Betydningen for den jødiske fa
- Page 41 and 42: af medicinske årsager, hvoraf alvo
- Page 43 and 44: lodtrækning fik foretaget omskære
- Page 45 and 46: Endvidere skal lægen i fornødent
- Page 47 and 48: Stritøreoperationer udføres både
- Page 49 and 50: Den foreliggende medicinske forskni
- Page 51 and 52: TECHNICAL REPORTMale Circumcisionab
- Page 53: principle on which each of thesedev
- Page 57 and 58: TABLE 2 Results from Medline, Cochr
- Page 59 and 60: Male Circumcision and Diseases,Morb
- Page 61 and 62: een diagnosed with genital herpes a
- Page 63 and 64: Results data indicate that the inci
- Page 65 and 66: participants’ ages and any coexis
- Page 67 and 68: without general anesthesia in boys
- Page 69 and 70: was reported in 2.2% of cases andin
- Page 71 and 72: nurse practitioners) should workcol
- Page 73 and 74: circumcision practices in theUnited
- Page 75 and 76: at: www.cdc.gov/hiv/resources/facts
- Page 77 and 78: childhood: a meta-analysis. Pediatr
- Page 79 and 80: multicenter survey. Isr Med Assoc J
- Page 81 and 82: Male CircumcisionTASK FORCE ON CIRC
- Page 83 and 84: The online version of this article,
- Page 85 and 86: COMMENTARYIn this commentary, a dif
- Page 87 and 88: COMMENTARYThe cardinal medical ques
- Page 89 and 90: Cultural Bias in the AAP's 2012 Tec
- Page 91 and 92: Weiss et al. BMC Urology 2010, 10:2
- Page 93 and 94: Weiss et al. BMC Urology 2010, 10:2
- Page 95 and 96: Weiss et al. BMC Urology 2010, 10:2
- Page 97 and 98: Weiss et al. BMC Urology 2010, 10:2
- Page 99 and 100: Weiss et al. BMC Urology 2010, 10:2
- Page 101 and 102: Weiss et al. BMC Urology 2010, 10:2
- Page 103 and 104: 2013-06-21 Dnr x.x-xxxxx/xxxx 1(4)T
- Page 105 and 106:
SOCIALSTYRELSEN 2013-06-21 Dnr 3(4)